


Sexually transmitted infections (STIs) and HIV have a known correlation with the presence of either one increasing the risk for the other. Data have shown that the presence of an STI increases the chance of HIV acquisition when those individuals engage in unsafe sex practices and have contact with people with HIV who have a detectable viral load. The proposed mechanism for the increased risk for HIV acquisition is damage to epithelial tissue from genital ulcers or a break in the skin increasing the risk for HIV transmission during sex with a person whose HIV is not well controlled. Individuals with detectable HIV viral loads have a higher chance of shedding virus, especially if they have concomitant urethritis or genital ulcers. Conversely, the presence of HIV also increases the risk for infections with other STIs likely due to continued engagement in unsafe behaviors.1
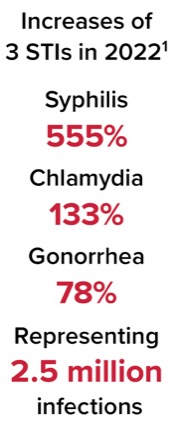
Rates of STIs including syphilis, gonorrhea, and chlamydia have increased significantly over the last few years, with 2.5 million new cases in 2022 alone representing increases of 555% for syphilis, 133% for chlamydia, and 78% for gonorrhea. When looking at the effect these increases have on coinfection with HIV, data have demonstrated that about 6% of sexually acquired HIV is linked to those 3 infections. There is also a significant economic burden associated with this increase, with the lifetime medical costs of new HIV infections totaling $800 million for approximately 1,800 new infections.1
When looking at the correlation between the STIs and HIV acquisition, the rate of HIV acquisition varies based on the concurrent STI. In addition to the more common STIs, there is a significant increase that has been observed in some of the lesser known STIs. This article will review some of the STIs that have increased significantly over the past several years and discuss the importance of collaboration among healthcare professionals, patient advocates, federal and local governments, and patients on addressing the increasing prevalence of STIs and HIV infection.
Syphilis
Reported in 2022, the incidence of syphilis has increased rapidly with 207,255 cases, inclusive of all stages and congenital syphilis, representing an increase of 17.3% in 1 year. The rising rates have been steady since 2000. These escalations have been observed regardless of age, gender, and geographic location.1
The rates of syphilis have increased in both women and men who have sex with men (MSM), with the latter population representing a significant proportion, 45.1%, of all cases of primary and secondary syphilis in men in 2022. Data from Florida in 2003 demonstrated that 42% of all patients diagnosed with syphilis were also coinfected with HIV. Those who identify as MSM with a history of syphilis are more likely to acquire HIV infection compared with those who have not tested positive for syphilis. Twenty-two percent of MSM who were diagnosed with syphilis in Florida in 2003 subsequently tested positive for HIV by 2011.1
Gonorrhea/Chlamydia
Historical data have demonstrated that individuals who have a history of rectal gonorrhea or chlamydia have an increased risk for acquiring HIV (Table 1). Additional data have estimated that about 10% of new HIV infections in MSM could be linked to gonorrhea/chlamydia infections, accounting for about 2,600 new HIV cases annually.1
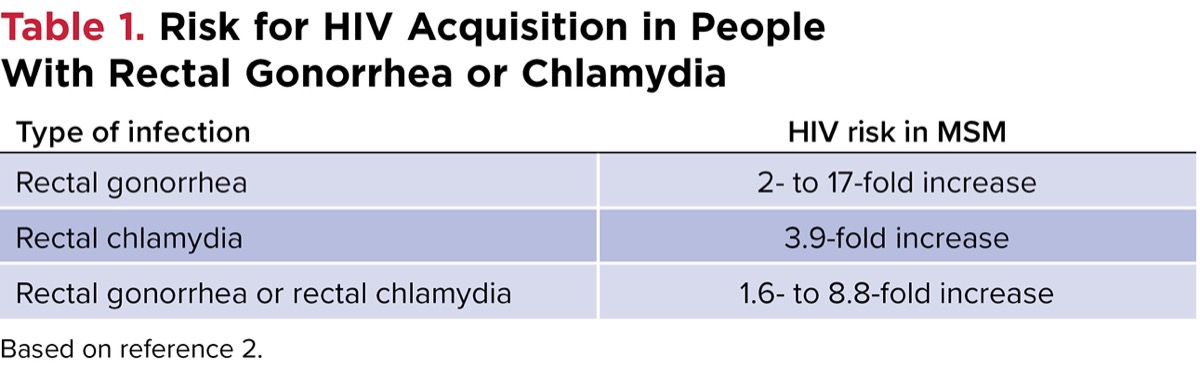
| Table 1. Risk for HIV Acquisition in People With Rectal Gonorrhea or Chlamydia | |
| Type of infection | HIV risk in MSM |
|---|---|
| Rectal gonorrhea | 2- to 17-fold increase |
| Rectal chlamydia | 3.9-fold increase |
| Rectal gonorrhea or rectal chlamydia | 1.6- to 8.8-fold increase |
| Based on reference 2. | |
Barbee and colleagues conducted a stratified case-control study to investigate this association and determine if the correlation between rectal STIs and HIV acquisition is still present after accounting for sexual behavior. A total of 176 cases—MSM with new HIV (positive test within prior 12 months), and 704 controls, MSM without HIV (negative test within 12 months)—were included for evaluation. At the time of their HIV test visit, both case and control patients had negative results on syphilis and rectal STI tests. Notably, the authors excluded individuals who had syphilis at the time of enrollment due to the known association with HIV acquisition. Both case and control patients were categorized based on their receptive anal intercourse practices in 1 of the following groups:
- no receptive anal intercourse; condom use for all receptive anal intercourse;
- condomless receptive anal intercourse with HIV-negative partners only; or
- condomless receptive anal intercourse with HIV-positive partners or partners with unknown HIV status.
After characterizing patients, the authors created logistic regression models to calculate the attributable risk of rectal STIs for HIV acquisition. They found that both rectal gonorrhea and chlamydia were associated with an increased incidence of HIV, with associated odds ratio of 3.0 (95% CI, 1.5-6.2) for rectal gonorrhea or chlamydia. Specific associations are listed in Table 2. The authors concluded that in the MSM population, rectal STIs contributed to 1 in 7 new HIV diagnoses. Through an exploratory analysis, the presence or history of rectal STIs increased the risk for new HIV diagnoses by 3.8 (P=0.013).2
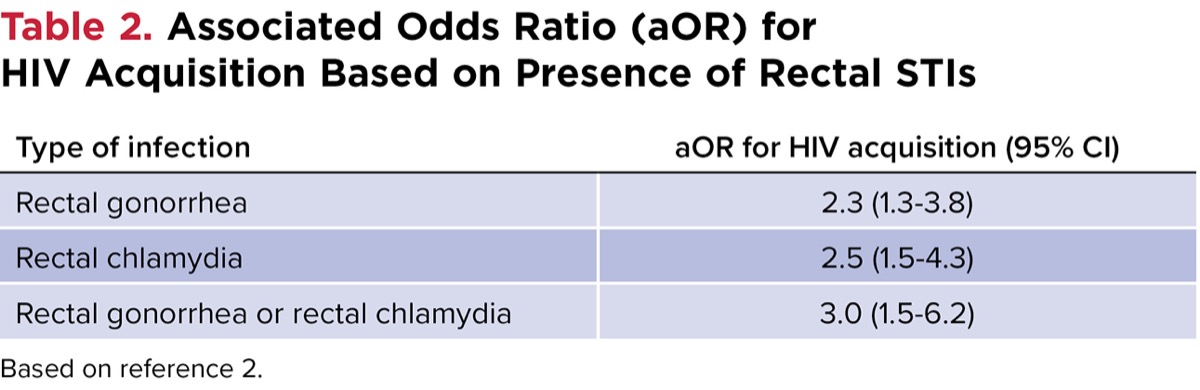
| Table 2. Associated Odds Ratio (aOR) for HIV Acquisition Based on Presence of Rectal STIs | |
| Type of infection | aOR for HIV acquisition (95% CI) |
|---|---|
| Rectal gonorrhea | 2.3 (1.3-3.8) |
| Rectal chlamydia | 2.5 (1.5-4.3) |
| Rectal gonorrhea or rectal chlamydia | 3.0 (1.5-6.2) |
| Based on reference 2. | |
Mycoplasma genitalium
Mycoplasma genitalium is a growing concern across the United States due to the development of antimicrobial resistance and limited options for treatment, which put it on the CDC Watch List for Antimicrobial Resistance Threats.
Related Content



Manhart and colleagues implemented a surveillance program to identify the estimated prevalence of M. genitalium due to a lack of population estimates in individuals at higher risk for STIs. Data prior to their evaluation sampled patients through the National Health and Nutrition Examination Survey in 2017-2018, which reported 1.7% prevalence of M. genitalium.3 The surveillance program implemented by Manhart and colleagues included sexual health clinics in 4 different geographic regions to estimate the true prevalence of M. genitalium and incidence of antimicrobial resistance in these populations.
More than 1,700 specimens were collected, with 993 specimens from males and 750 specimens from females. M. genitalium was detected in 16.6% (95% CI, 14.9%-18.5%) of specimens. Prevalence rates were higher in females at 17.6% vs 15.9%, but there were no significant differences found when comparing people with same-sex partners and those with opposite-sex partners. Rates in this surveillance database were approximately 10 times higher than the numbers reported from 2017-2018.4
This increased incidence of M. genitalium is especially concerning in the setting of the rise in macrolide-resistant isolates and highlights the importance of evaluation/testing for M. genitalium especially in people with HIV.
Federal Plan for STIs
In response to the increasing incidence of STIs in the United States, the federal government developed an STI implementation plan to decrease the number of new STIs by 2025 and 2030. This plan highlights the importance of implementing strategies to reduce the risk for acquisition of STIs and HIV. Approaches to prevent HIV acquisition include optimizing the use of antiretrovirals to increase the number of people with undetectable viral loads, thus preventing transmission of HIV to serodiscordant partners. An additional HIV prevention measure involves using pre- or post-exposure prophylaxis in people with negative HIV tests who engage in unsafe sexual behaviors.5
References
- Centers for Disease Control and Prevention. STI Surveillance, 2022. Accessed May 31, 2024. https://bit.ly/ 453L8qm-IDSE
- Barbee LA, Khosropour CM, Dombrowksi JC, et al. Sex Transm Dis. 2017;44(7):385-389.
- Torrone EA, Kruszon-Moran D, Philips C, et al. Sex Transm Dis. 2021;48(11):e160-e162.
- Manhart LE, Leipertz G, Soge OO, et al. Clin Infect Dis. 2023;77(10):1449-1459.
- US Department of Health and Human Services. STI National Strategic Plan. Sexually Transmitted Infections National Strategic Plan. 2023. Accessed May 30, 2024. https://bit.ly/ 3Vl7qAF-idse
About the author:

Copyright © 2024 McMahon Publishing, 545 West 45th Street, New York, NY 10036. Printed in the USA. All rights reserved, including the right of reproduction, in whole or in part, in any form.

Download to read this article in PDF document:![]() Sexually Transmitted Infections and HIV: Opportunities
Sexually Transmitted Infections and HIV: Opportunities