


Although antimicrobials are prescribed frequently to the general population in both the community and hospital setting, they may be prescribed inappropriately at a higher rate in people with HIV due to their increased contact with the healthcare system, especially in patients with more pronounced immunosuppression. This is demonstrated in a retrospective evaluation through the HIV Virtual Cohort Study that was conducted by Sweet et al in which they evaluated the rate of antimicrobial prescribing in people with HIV (PWH) and those without HIV in patients with acute respiratory tract infections. Antimicrobials were prescribed less frequently overall in PWH (26%) compared with those without HIV (34%); however, there was a higher rate of inappropriate antimicrobial prescribing in PWH versus those without HIV.1
The increased use of antimicrobials can lead to the development of antimicrobial resistance, which already is associated with almost 3 million infections and 35,000 deaths as of 2019.2 Ford et al reviewed the current literature to determine what factors contributed to hospital admission and mortality in PWH worldwide. The data demonstrated that bacterial infections were the second-leading cause of hospitalization and mortality in adult patients, second only to AIDS-related illnesses.3
Antimicrobials account for a significant amount of medication expenditures, totaling $56 billion from 2010 through 2015, with just more than half of those expenditures (59.1%) accounting for antimicrobials prescribed in the outpatient setting.4 When looking at the number of antimicrobials prescribed, upward of 90% of antimicrobials are prescribed in the community/outpatient setting. Over the 5-year period, approximately 236 million people received antimicrobial prescriptions, meaning that antimicrobials are being prescribed to 7 of every 10 patients in the United States. Data have demonstrated that almost 30% of these antimicrobials are unnecessary.5
Use of unnecessary antimicrobials can lead to significant adverse outcomes, such as antimicrobial resistance and Clostridioides difficile infection (CDI). Despite the decreased incidence of CDI overall, there was a significant increase in the incidence of community-acquired CDI over the period of 2011 to 2017 from 170,000 cases to 462,100 cases annually.6

Kong et al evaluated the different rates of medication prescribing, including antimicrobials in PWH ages 65 years and older. The results of the evaluation demonstrated that older PWH had slightly higher rates of medications prescribed, including penicillins and macrolides, compared with those who were the same age without HIV.7
Effect of HIV on Risk for Antimicrobial Resistance
After assessing patients and identifying signs and symptoms for infection, the next step is to determine the most appropriate antimicrobial therapy to initiate. When selecting antimicrobials, it is important to consider several factors: the causative organism, treatment indication, antimicrobial susceptibility (regionally and nationally, as well as patient-specific microbiology), and other patient-specific factors such as allergies, concurrent medications, and relevant laboratory values.
Olaru et al conducted a systematic review and meta-analysis to determine how the incidence of antimicrobial resistance affected PWH.8 Across 92 studies, approximately 40,000 PWH and just fewer than 17 million without HIV were included in the analysis. For PWH, CD4+ counts were included in 39 of the 92 studies, with median CD4+ counts above 200 cells/mm3 in 64% of the 39 studies, whereas median CD4+ counts were below 200 cells/mm3 in the 53 remaining. Pooled analyses demonstrated some differences regarding antimicrobial susceptibility for those with and without HIV (Table 1).8 These results demonstrate that PWH may have an increased rate of resistance compared with the general population; however, the included trials were of low to moderate quality, and the pooled analysis did not allow for evaluation based on degree of immunosuppression.
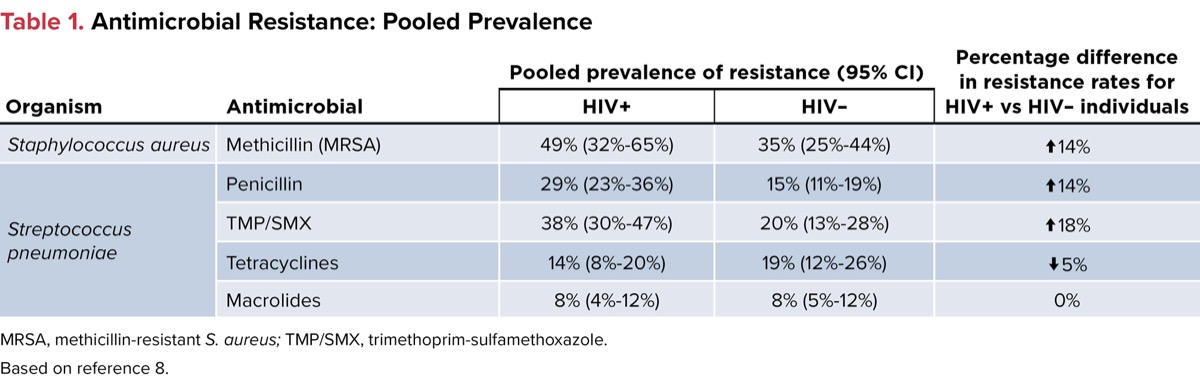
| Table 1. Antimicrobial Resistance: Pooled Prevalence | ||||
| Organism | Antimicrobial | Pooled prevalence of resistance (95% CI) | Percentage difference in resistance rates for HIV+ vs | |
|---|---|---|---|---|
| HIV+ | HIV– | |||
| Staphylococcus aureus | Methicillin (MRSA) | 49% (32%-65%) | 35% (25%-44%) | |
| Streptococcus pneumoniae | Penicillin | 29% (23%-36%) | 15% (11%-19%) | |
| TMP/SMX | 38% (30%-47%) | 20% (13%-28%) | ||
| Tetracyclines | 14% (8%-20%) | 19% (12%-26%) | ||
| Macrolides | 8% (4%-12%) | 8% (5%-12%) | 0% | |
| MRSA, methicillin-resistant S. aureus; TMP/SMX, trimethoprim-sulfamethoxazole. Based on reference 8. | ||||
Related Content



Choice of Empiric Antimicrobials
Antimicrobial choice in patients with community-acquired pneumonia should be consistent regardless of a patient’s HIV status. The Department of Health and Human Services guidelines recommend that respiratory cultures and specimens, if being collected, ideally should be collected prior to the administration of antimicrobial therapy; however, if indicated, antimicrobials should be administered promptly.9
Recommendations for empiric coverage should consider antimicrobial resistance, as discussed above, severity of disease, and methicillin-resistant Staphylococcus aureus (MRSA) and pseudomonal risk factors. Historically, PWH had been at higher risk for Pseudomonas aeruginosa. However, with the advent of antiretroviral therapy, that risk has diminished significantly. Those with advanced HIV and CD4+ counts less than 50 cells/mm3 remain at increased risk for P. aeruginosa, otherwise those with CD4+ counts above 50 cells/mm3 have a similar risk for pseudomonal infection as the general population. S. aureus risk factors in PWH are similar to that of the general population and include recent healthcare exposure or antimicrobial exposure, as well as recent viral infections. Studies have demonstrated that PWH are more likely to be colonized with MRSA compared with the general population, especially in the nasal carriages and on the skin (Table 2).9
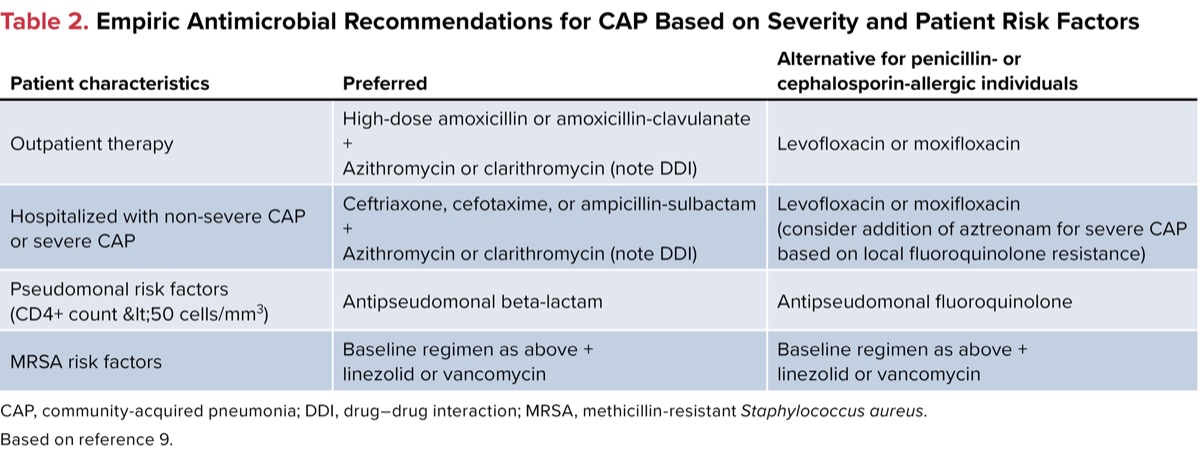
| Table 2. Empiric Antimicrobial Recommendations for CAP Based on Severity and Patient Risk Factors | ||
| Patient characteristics | Preferred | Alternative for penicillin- or cephalosporin-allergic individuals |
|---|---|---|
| Outpatient therapy | High-dose Amoxicillin/17602" target="_blank">amoxicillin or amoxicillin-clavulanate + Azithromycin or clarithromycin (note DDI) | Levofloxacin or moxifloxacin |
| Hospitalized with | Ceftriaxone, cefotaxime, or ampicillin-sulbactam + Azithromycin or clarithromycin (note DDI) | Levofloxacin or moxifloxacin (consider addition of aztreonam for severe CAP based on local fluoroquinolone resistance) |
| Pseudomonal risk factors (CD4+ count | Antipseudomonal | Antipseudomonal fluoroquinolone |
| MRSA risk factors | Baseline regimen as above + linezolid or vancomycin | Baseline regimen as above + linezolid or vancomycin |
| CAP, community-acquired pneumonia; DDI, drug–drug interaction; MRSA, methicillin-resistant Staphylococcus aureus. Based on reference 9. | ||
Strategies for Reducing Antimicrobial Resistance
Strategies that are employed through antimicrobial stewardship in the general population can also be applied to those with HIV. The CDC has several strategies that can be implemented to decrease the incidence or emergence of antimicrobial resistance. These strategies include: 1) preventing infections and decreasing the spread by use of vaccinations; 2) implementing routine screening in at-risk groups and treatment as indicated; 3) ensuring appropriate preparation and safe handling of food; and 4) optimizing antimicrobial use. These strategies, especially the use of vaccinations, appropriate screening, and optimizing antimicrobial use, are essential to reduce the risk for preventable infections and antimicrobial resistance developing among those with and without HIV.

In addition to the strategies proposed by the CDC, healthcare providers can also focus on the 5 R’s of antimicrobial prescribing: right patient, right time, right drug, right dose, and right duration. Careful evaluation of the 5 R’s can help aid optimal initiation and selection of antimicrobials in individuals with and without HIV (Figure). With an increasing rate of antimicrobial prescribing and resistance, it is critical that healthcare providers assess the need for and choice of antimicrobial therapy in all patients, especially those with HIV.
References
- Sweet L, Daniels C, Xu X, et al. Acute respiratory infection incidence and outpatient antibiotic prescription patterns in people with or without human immunodeficiency virus infection: a virtual cohort study. Open Forum Infect Dis. 2023;10(7):ofad272.
- CDC. Antibiotic Resistance Threats in the United States, 2019. Department of Health and Human Services, CDC; 2019. Accessed July 21, 2025. cdc.gov/antimicrobial-resistance/data-research/threats/index.html
- Ford N, Shubber Z, Meintjes G, et al. Causes of hospital admission among people living with HIV worldwide: a systematic review and meta-analysis. Lancet HIV. 2015;2(10):e438-e444.
- Suda KJ, Hicks LA, Roberts RM, et al. Antibiotic expenditures by medication, class, and healthcare setting in the United States, 2010-2015. Clin Infect Dis. 2018;66(2):185-190.
- Hersh AL, King LM, Shapiro DJ, et al. Unnecessary antibiotic prescribing in US ambulatory care settings, 2010-2015. Clin Infect Dis. 2021;72(1):133-137.
- Fu Y, Luo Y, Grinspan AM. Epidemiology of community-acquired and recurrent Clostridioides difficile infection. Therap Adv Gastroenterol. 2021;14:17562848211016248.
- Kong AM, Pozen A, Anastos K, et al. Non-HIV comorbid conditions and polypharmacy among people living with HIV age 65 or older compared with HIV-negative individuals age 65 or older in the United States: a retrospective claims-based analysis. AIDS Patient Care STDs. 2019;33(3):93-103.
- Olaru ID, Tacconelli E, Yeung S, et al. The association between antimicrobial resistance and HIV infection: a systematic review and meta-analysis. Clin Microbiol Infect. 2021;27(6):846-853.
- Panel on guidelines for the prevention and treatment of opportunistic infections in adults and adolescents with HIV. Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents With HIV. Updated July 14, 2025. Accessed July 21, 2025. clinicalinfo.hiv.gov/en/guidelines/adult-and-adolescent-opportunistic-infection
About the author:

Copyright © 2025 McMahon Publishing, 545 West 45th Street, New York, NY 10036. Printed in the USA. All rights reserved, including the right of reproduction, in whole or in part, in any form.

Download to read this article in PDF document:![]() Antimicrobial Stewardship in Community-Acquired Pneumonia: Considerations in People With HIV
Antimicrobial Stewardship in Community-Acquired Pneumonia: Considerations in People With HIV