


Antimicrobial resistance (AMR) poses a major global health threat and is strongly associated with increased morbidity and mortality rates worldwide.1-3 The CDC estimates that nearly 3 million AMR infections occur each year in the United States, resulting in approximately 35,000 deaths.3 According to this report, carbapenem-resistant Acinetobacter is classified as an urgent threat, with an estimated 8,500 cases and 700 deaths annually.3
Carbapenem-resistant Acinetobacter baumannii (CRAB) exhibits a broad array of resistance mechanisms, including the production of beta-lactamases such as OXA-type enzymes (eg, OXA-23, OXA-24/40, and OXA-51), which confer resistance to beta-lactam antibiotics. In addition, mutations in penicillin-binding proteins (PBPs), including PBP1 and PBP3, can contribute further to sulbactam resistance.4-7 Beyond these mechanisms of resistance, A. baumannii requires alternative strategies such as the loss or modification of outer membrane porins and active extrusion of antibiotics via efflux pumps.8
With the increasing prevalence of CRAB infections and limited availability of safe and effective therapeutic options, an evaluation of current treatment strategies is warranted. Of note, the general strategy in the management of CRAB infections involves the use of combination antimicrobial therapy with at least 2 agents, with suggestion to use one agent that is sulbactam-based, until an appropriate clinical response is observed.4 Some examples of traditionally used agents include high-dose ampicillin-sulbactam, high-dose carbapenems, polymyxins, and/or tetracycline derivatives.4,9 Regarding the non–beta-lactam agents, polymyxins are less favored because of their unpredictable pharmacokinetics and significant risks for nephrotoxicity and neurotoxicity.10,11 Concerns with the tetracycline derivatives include rapid tissue distribution leading to limited serum and urine concentrations.4,12
Ampicillin-sulbactam, a beta-lactam/beta-lactamase inhibitor combination, has been a cornerstone for CRAB infections, primarily due to the intrinsic activity of sulbactam and the long-standing availability of ampicillin-sulbactam. Specifically, sulbactam exerts its antibacterial effect by saturating PBP1 and PBP3, and previous studies have identified sulbactam-containing regimens as demonstrating improved outcomes compared with alternative regimens.4,7,13,14 The recommended high-dose regimen in patients with normal renal function includes a total daily dose of 9 g of sulbactam, either as a 4-hour infusion of 9 g of ampicillin-sulbactam (6 g ampicillin, 3 g sulbactam) every 8 hours or a 24-hour continuous infusion of 27 g of ampicillin-sulbactam (18 g ampicillin, 9 g sulbactam). However, the increasing prevalence of resistance, including mechanisms not mediated by PBPs, has prompted the exploration of novel therapeutic strategies aimed at overcoming these limitations.4
In May 2023, the FDA approved sulbactam-durlobactam (SUL-DUR; Xacduro, Innoviva), a novel combination of two beta-lactamase inhibitors, in patients at least 18 years of age for the treatment of hospital-acquired and ventilator-associated bacterial pneumonia (HABP/VABP) caused by susceptible isolates of A. baumannii-calcoaceticus complex (ABC). Specifically, SUL-DUR is administered as a fixed dose in a 1:1 ratio with a total daily dose of 2 g (1 g sulbactam, 1 g durlobactam) every 6 hours as a 3-hour infusion.15 According to the Infectious Diseases Society of America 2024 guidance document on AMR gram-negative infections, SUL-DUR is the preferred agent for the treatment of CRAB infections in combination with a carbapenem (meropenem or imipenem-cilastatin) supported by in vitro, pharmacokinetic/pharmacodynamic, and clinical data demonstrating safety and efficacy for ABC isolates.4,16-18 A comparison of SUL-DUR and ampicillin-sulbactam in treating CRAB is provided in the Table.4,15,19
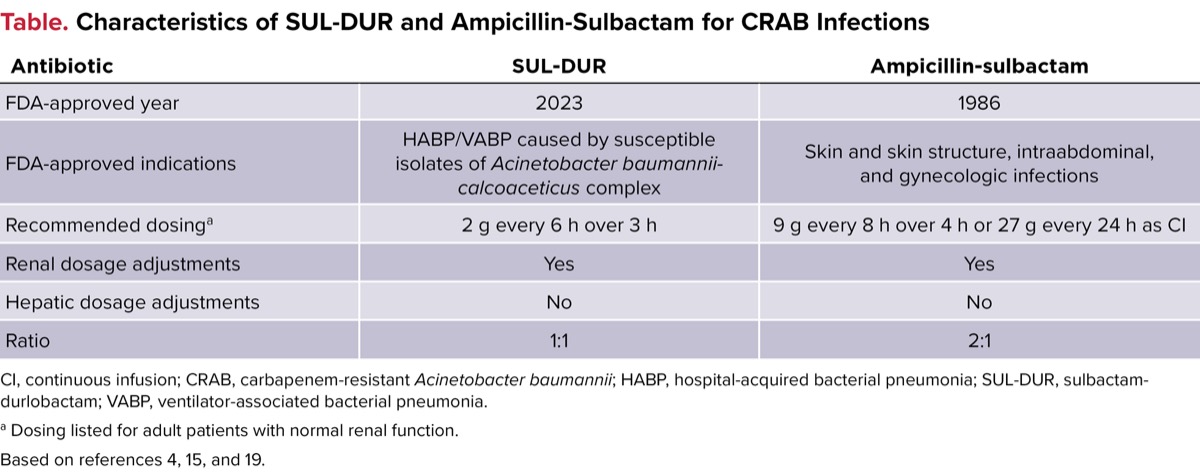
| Table. Characteristics of SUL-DUR and Ampicillin-Sulbactam for CRAB Infections | ||
| Antibiotic | SUL-DUR | Ampicillin-sulbactam |
|---|---|---|
| FDA-approved year | 2023 | 1986 |
| FDA-approved indications | HABP/VABP caused by susceptible isolates of Acinetobacter baumannii-calcoaceticus complex | Skin and skin structure, intraabdominal, and gynecologic infections |
| Recommended dosinga | 2 g every 6 h over 3 h | 9 g every 8 h over 4 h or 27 g every 24 h as CI |
| Renal dosage adjustments | Yes | Yes |
| Hepatic dosage adjustments | No | No |
| Ratio | 1:1 | 2:1 |
| CI, continuous infusion; CRAB, carbapenem-resistant Acinetobacter baumannii; HABP, hospital-acquired bacterial pneumonia; SUL-DUR, sulbactam-durlobactam; VABP, ventilator-associated bacterial pneumonia. a Dosing listed for adult patients with normal renal function. Based on references 4, 15, and 19. | ||
The primary purpose of this review is to summarize the in vitro and clinical evidence for Acinetobacter spp and CRAB infections, with a focus on SUL-DUR.
Overview of SUL-DUR In Vitro studies
Sulbactam exhibits intrinsic antibacterial activity through its binding to PBP1 and PBP3; however, its efficacy is compromised by enzymatic degradation. The addition of durlobactam, a potent inhibitor of class A, C, and D beta-lactamases, services a critical role in preserving sulbactam’s activity. By inhibiting these beta-lactamases, durlobactam protects sulbactam from hydrolysis, thereby, enabling it to reach and bind its PBP targets effectively. This mechanism significantly enhances the in vitro activity of the SUL-DUR combination against CRAB isolates and allows for the use of lower sulbactam doses compared with ampicillin-sulbactam.4,16,20
Related Content



Karlowsky and colleagues conducted an in vitro analysis to evaluate the activity of SUL-DUR against ABC, testing 5,032 isolates collected from 33 countries between 2016 and 2021.16 Of importance, most were A. baumannii (80.2%), followed by A. pittii (12.7%), A. nosocomialis (5.9%), and A. calcoaceticus (1.1%). Susceptibility testing was performed following the Clinical and Laboratory Standards Institute (CLSI) guidelines using the microdilution method with 2-fold dilutions of sulbactam and a fixed durlobactam concentration of 4 mg/L with a susceptible minimum inhibitory concentration (MIC) breakpoint of 4/4 mg/L. SUL-DUR demonstrated potent activity, with MIC50 and MIC90 (ie, MIC inhibition of 50% and 90%) values of 1 and 2 mg/L, respectively, across all isolates. Of note, the addition of durlobactam to sulbactam reduced its MIC90 by 32-fold (from 64 to 2 mg/L) for all ABC isolates. At the CLSI susceptibility breakpoint of 4/4 mg/L, SUL-DUR inhibited 98.3% of all ABC isolates.21 Furthermore, SUL-DUR exhibited high rates of susceptibility across sulbactam–non-susceptible (96.9%; n=2,670) and imipenem–non-susceptible (96.7%; n=2,570) isolates. Of the 1.7% of total ABC isolates with MIC values that exceeded the breakpoint, these resistance mechanisms likely were associated primarily with PBP3 mutations and/or the presence of metallo-beta-lactamases (MBLs).16
Another in vitro evaluation was conducted by Findlay and colleagues that involved 100 carbapenemase-producing A. baumannii isolates.20 Susceptibility testing was performed using the CLSI broth microdilution method with a SUL-DUR susceptible MIC breakpoint of 4/4 mg/L. This collection included producers of OXA-23 (n=73), OXA-72 (n=10), OXA-40 (n=6), OXA-58 (n=5), and OXA-24 (n=1), as well as New Delhi MBL producers (n=5). Overall, 71.0% of isolates were susceptible to SUL-DUR, compared with 3.0% and 46.0% of isolates exhibiting susceptibility to sulbactam and minocycline, respectively.20
ATTACKing CRAB With SUL-DUR
Kaye and colleagues conducted the ATTACK study, which was a phase 3, multicenter, randomized, active-controlled, noninferiority trial to assess the safety and efficacy of SUL-DUR compared with colistin in hospitalized patients with confirmed serious infections (HABP/VABP, ventilated pneumonia, or bloodstream infections) due to ABC, including carbapenem-resistant strains (Figure).18 Patients were randomized 1:1 to receive SUL-DUR (2 g every 6 hours infused over 3 hours) or colistin (2.5 mg/kg every 12 hours infused over 30 minutes) in combination with imipenem-cilastatin (2 g every 6 hours infused over 1 hour) as background therapy for 7 to 14 days. The investigators concluded that noninferiority was established if the upper limit of the 2-sided 95% CI for the treatment difference did not exceed 20%.
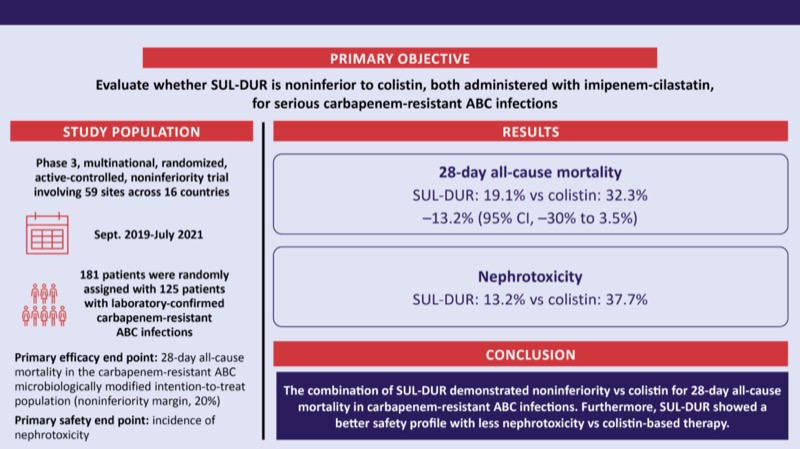
The researchers randomly assigned 181 patients, with 125 patients with laboratory-confirmed carbapenem-resistant ABC being included within the primary efficacy analysis (SUL-DUR, 50.4% vs colistin, 49.6%). There were no major differences in Charlson Comorbidity Index, APACHE II (Acute Physiology and Chronic Health Evaluation II) scores, those requiring mechanical ventilation, and infection types (which were primarily HABP/VABP). The primary efficacy end point of 28-day all-cause mortality occurred in 19.1% of the SUL-DUR group compared with 32.3% in the colistin group, a difference of –13.2% (95% CI, –30.0% to 3.5%), meeting the noninferiority margin. SUL-DUR was also associated with substantial improvements in microbiological favorable response and clinical cure. Furthermore, the incidence of nephrotoxicity was significantly lower in the SUL-DUR group compared with colistin (13.2% vs 37.7%; P<0.001), whereas serious adverse events were numerically lower in the SUL-DUR group (39.6% vs 48.8%).18
Conclusion
CRAB remains a formidable public health threat due to its multifaceted resistance mechanisms and limited treatment options.2,4 The emergence of SUL-DUR represents a significant advancement in the therapeutic landscape, offering targeted inhibition of selected beta-lactamases and restoration of sulbactam’s intrinsic activity against key PBPs.4,16 In vitro data demonstrate potent activity across diverse Acinetobacter spp isolates, including those resistant to sulbactam and carbapenems, while clinical evidence from the ATTACK trial demonstrated SUL-DUR’s noninferiority to colistin with markedly reduced nephrotoxicity.16,18,20 These data mark a pivotal shift toward more efficacious and safer treatment strategies for this urgent antimicrobial resistance threat.4
References
- Christaki E, Marcou M, Tofarides A. Antimicrobial resistance in bacteria: mechanisms, evolution, and persistence. J Mol Evol. 2020;88(1):26-40.
- About antimicrobial resistance. CDC. Published January 31, 2025. Accessed September 5, 2025. cdc.gov/antimicrobial-resistance/about/index.html
- CDC. Antibiotic Resistance Threats in the United States, 2019. US Department of Health and Human Services, CDC; 2019. cdc.gov/antimicrobial-resistance/data-research/threats/index.html
- Tamma PD, Heil EL, Justo JA, et al. Infectious Diseases Society of America 2024 guidance on the treatment of antimicrobial-resistant gram-negative infections. Clin Infect Dis. Published online August 7, 2024. doi:10.1093/cid/ciae403
- McKay SL, Vlachos N, Daniels JB, et al. Molecular characterization of carbapenem- resistant Acinetobacter baumannii in the United States, 2013-2017. Microb Drug Resist. 2022;28(6):645-653.
- Carbapenem-resistant Acinetobacter baumannii (CRAB): an urgent public health threat in United States healthcare facilities. CDC. Antimicrobial Resistance & Patient Safety Portal. Published August 2021. Accessed September 5, 2025. arpsp.cdc.gov/story/cra-urgent-public-health-threat
- Penwell WF, Shapiro AB, Giacobbe RA, et al. Molecular mechanisms of sulbactam antibacterial activity and resistance determinants in Acinetobacter baumannii. Antimicrob Agents Chemother. 2015;59(3):1680-1689.
- Kyriakidis I, Vasileiou E, Pana ZD, et al. Acinetobacter baumannii antibiotic resistance mechanisms. Pathogens. 2021;10(3):373.
- Abdul-Mutakabbir JC, Griffith NC, Shields RK, et al. Contemporary perspective on the treatment of Acinetobacter baumannii infections: insights from the Society of Infectious Diseases Pharmacists. Infect Dis Ther. 2021;10(4):2177-2202.
- Avedissian SN, Liu J, Rhodes NJ, et al. A review of the clinical pharmacokinetics of polymyxin B. Antibiotics (Basel). 2019;8(1):31.
- Wagenlehner F, Lucenteforte E, Pea F, et al. Systematic review on estimated rates of nephrotoxicity and neurotoxicity in patients treated with polymyxins. Clin Microbiol Infect. Published online January 6, 2021. doi:10.1016/j.cmi.2020.12.009
- Agwuh KN, MacGowan A. Pharmacokinetics and pharmacodynamics of the tetracyclines including glycylcyclines. J Antimicrob Chemother. 2006;58(2):256-265.
- Liu J, Shu Y, Zhu F, et al. Comparative efficacy and safety of combination therapy with high-dose sulbactam or colistin with additional antibacterial agents for multiple drug-resistant and extensively drug-resistant Acinetobacter baumannii infections: a systematic review and network meta-analysis. J Glob Antimicrob Resist. 2021;24:136-147.
- Jung SY, Lee SH, Lee SY, et al. Antimicrobials for the treatment of drug-resistant Acinetobacter baumannii pneumonia in critically ill patients: a systemic review and Bayesian network meta-analysis. Crit Care. 2017;21(1):319.
- Xacduro. Package insert. Entasis Therapeutics/Innoviva; May 23, 2023. Accessed September 5, 2025. accessdata.fda.gov/drugsatfda_docs/label/2023/216974Orig1s000Correctedlbl.pdf
- Karlowsky JA, Hackel MA, McLeod SM, et al. In vitro activity of sulbactam-durlobactam against global isolates of Acinetobacter baumannii-calcoaceticus complex collected from 2016 to 2021. Antimicrob Agents Chemother. 2022;66(9):e0078122.
- O’Donnell JP, Bhavnani SM. The pharmacokinetic/pharmacodynamic relationship of durlobactam in combination with sulbactam in in vitro and in vivo infection model systems versus Acinetobacter baumannii-calcoaceticus complex. Clin Infect Dis. 2023;76(suppl 2):S202-S209.
- Kaye KS, Shorr AF, Wunderink RG, et al. Efficacy and safety of sulbactam-durlobactam versus colistin for the treatment of patients with serious infections caused by Acinetobacter baumannii-calcoaceticus complex: a multicentre, randomised, active-controlled, phase 3, non-inferiority clinical trial (ATTACK). Lancet Infect Dis. 2023;23(9):1072-1084.
- Unasyn. Package insert. Pfizer; January 31, 2025. Accessed September 5, 2025. accessdata.fda.gov/drugsatfda_docs/label/2025/050608s056lbl.pdf
- Findlay J, Poirel L, Bouvier M, et al. In vitro activity of sulbactam-durlobactam against carbapenem-resistant Acinetobacter baumannii and mechanisms of resistance. J Glob Antimicrob Resist. 2022;30:445-450.
- Clinical and Laboratory Standards Institute (CLSI). CLSI M100: Performance Standards for Antimicrobial Susceptibility Testing. 35th ed. CLSI; 2025.
About the authors:


Copyright © 2025 McMahon Publishing, 545 West 45th Street, New York, NY 10036. Printed in the USA. All rights reserved, including the right of reproduction, in whole or in part, in any form.

Download to read this article in PDF document:![]() Carbapenem-Resistant Acinetobacter baumannii: A Focus on Sulbactam-Durlobactam
Carbapenem-Resistant Acinetobacter baumannii: A Focus on Sulbactam-Durlobactam