


Antimicrobial resistance (AMR) is an international public health threat and a leading cause of mortality.1,2 In fact, the CDC has released the “2019 Antibiotic Resistance Threats Report,” which includes national infection and death estimates for nearly 20 worrisome pathogens.3 These national estimates have risen from previous iterations released by the CDC and are increasing at dramatic rates internationally.1-4 The inappropriate and excessive use of antimicrobials is a primary driver that potentiates AMR, and understanding the burden of AMR locally is crucial to implementing informed decisions operationally and clinically.1,5
Antimicrobial stewardship programs (ASPs) have been described in a policy statement from the Infectious Diseases Society of America, Pediatric Infectious Diseases Society, and the Society for Healthcare Epidemiology of America as “coordinated interventions designed to improve and measure the appropriate use of antimicrobial agents by promoting the selection of the optimal antimicrobial drug regimen including dosing, duration of therapy, and route of administration.”6 The development and implementation of ASPs have increased dramatically in recent decades; however, the term “ASP” was used traditionally in the narrow context of programs within individual inpatient settings or hospitals in which routine responsibilities included antimicrobial tracking, reporting, intervention (eg, prospective audit and feedback), and education.7,8
Although monitoring antimicrobial use throughout the inpatient setting is undoubtedly important, it has a limited effect on the outpatient setting where most antimicrobials are prescribed and misused.9,10 Unfortunately, ambulatory ASPs are not common in the United States, partly due to the fact that implementation of a comprehensive outpatient ASP is quite different than an inpatient ASP, given considerable differences in practice settings (Table).11,12 To assess the current state of ambulatory ASPs compared with inpatient ASPs, Eudy and colleagues conducted a recent cross-sectional, multicenter survey of Vizient member hospitals with ambulatory healthcare settings.11 Following receipt of 129 survey respondents from 44 states, a “fully functioning” ASP was present in only 7% of ambulatory practices compared with 88% of inpatient institutions.11
| Table. Comparison and Contrast of Inpatient And Outpatient Antimicrobial Stewardship Programs | ||
| Inpatient | Outpatient | |
| Duration of patient encounter | Days to weeks | Minutes |
| Internal control of antimicrobial dispensing and administration | ||
| Richness and availability of data | ||
| Patient follow-up | ||
While optimizing antimicrobial use, improving patient outcomes, and reducing the spread of AMR are the standard of care across inpatient and outpatient settings, different roads must be traveled to accomplish these goals effectively. The primary objective of this review is to describe national trends in outpatient antimicrobial prescribing, review the basic components and core elements of outpatient ASPs, and describe various strategies for managing ASP efforts in the outpatient setting.
Antimicrobial Use Is Not Just an Inpatient Problem
The CDC routinely performs outpatient antimicrobial prescription monitoring to analyze nationwide and state-specific trends to identify potential interventions directed at antimicrobial prescribing.9 Overall, it is estimated that between 80% and 90% of all human antibiotic consumption occurs in the outpatient setting.10 Of the prescribed antibiotics, 30% are deemed “completely unnecessary,” meaning no antibiotic was needed (eg, antibiotic prescribed for a viral respiratory infection), whereas 50% are deemed “inappropriate,” meaning the agent was either unnecessary or an incorrect therapeutic regimen prescribed (eg, wrong selection, dose, and/or duration).10,13 Many factors contribute to suboptimal antimicrobial prescribing in the ambulatory setting: provider time constraints, diagnostic uncertainty, delayed laboratory results, perceived patient and/or caregiver expectations for antimicrobials, patient satisfaction, fear of litigation if an infection is missed, and the possibility of limited patient follow-up.14,15
When evaluating outpatient antibiotic prescribing on the national level, healthcare professionals have prescribed between 200 and 250 million oral antibiotic prescriptions annually over recent years, and variability in prescribing is significant.16 These variations in antimicrobial prescribing are largely driven by the prescribing patterns of individual healthcare providers or specialty groups, independent of patients’ diagnoses.17 Of note, drastic variations in outpatient antibiotic prescribing also exist based on age group and geographic region. The rate of antibiotic prescriptions per 1,000 people is approximately 25% higher in adults at least 20 years of age compared with the pediatric population, whereas the rate of antibiotic prescribing has been reported to be highest in the southern regions (about 825 antibiotic prescriptions per 1,000 people) and lowest in the western regions (about 500 antibiotic prescriptions per 1,000 people).16

Based on provider and/or specialty group, the raw number of outpatient antibiotic prescriptions is led by physician assistants and nurse practitioners, followed by primary care physicians; however, the provider specialty responsible for the third highest antibiotic prescribing is dentistry at an estimated 25 million oral antibiotic prescriptions annually.16 When evaluating the rate of antibiotic prescriptions per provider, dermatology is responsible for the highest rate at about 300 prescriptions per provider, followed by emergency medicine at an estimated 180 prescriptions per provider. In comparison, physician assistants, nurse practitioners, and primary care physicians are responsible for an estimated 170 prescriptions per provider.16
An increase in ambulatory antibiotic consumption has given rise to community-onset infections exhibiting multidrug-resistant (MDR) phenotypes and/or increases in pathogenicity.18 Methicillin-resistant Staphylococcus aureus, a well-recognized, highly pathogenic organism, is one of the best examples of the MDR pathogen acquisition that has transitioned from being nearly nosocomial in nature to being widespread throughout the community.18,19 Also, the CDC’s 2019 resistance report cited above indicates that nearly half of extended-spectrum beta-lactamase–producing Enterobacterales infections occurred in the community setting without prior inpatient healthcare exposure or an invasive medical procedure.3 Other resistant phenotypes, such as MDR Neisseria gonorrhoeae, Streptococcus pneumoniae, and gastrointestinal pathogens (eg, Campylobacter spp, nontyphoidal Salmonella spp, and Shigella spp) almost exclusively begin in the community.18 Although the growth in ambulatory antibiotic prescribing and outpatient resistance rates is unfortunate, the increase has prompted governing organizations to create “standards” or “elements” for ambulatory ASPs.20,21
TJC and CDC Contributions
TJC Elements of Performance And CDC Core Elements
The sheer number of outpatient antimicrobial prescriptions coupled with the high rates of inappropriate prescribing and rising incidence of outpatient resistance rates underscore the importance of the development and implementation of ambulatory ASPs on the national, state, and local level. Consequently, in January 2020, The Joint Commission (TJC) requirements for ASPs in the ambulatory setting (TJC Standard MM.09.01.03) went into effect with 5 new elements of performance addressing ASPs in the outpatient setting (Figure 1).20 Furthermore, the CDC released the “Core Elements of Outpatient ASP,” which overlap with TJC elements of performance and include:
- commitment;
- action for policy and practice;
- tracking and reporting; and
- education and expertise.21
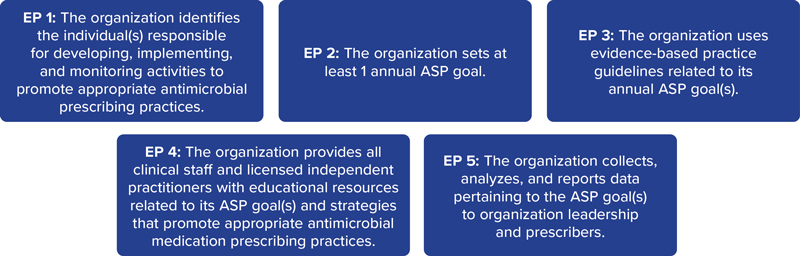
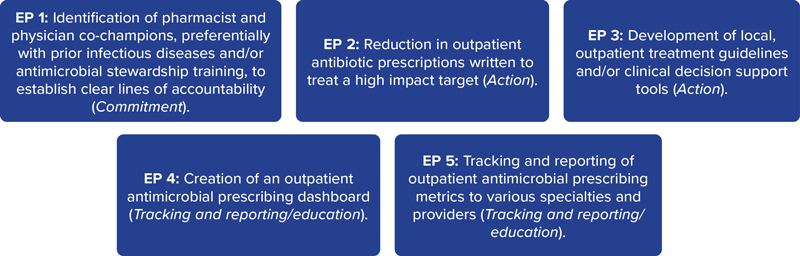
Figure 2 illustrates implementation strategies of these elements of performance and core elements, while other methods are described below.12,20,21
Practical Methods for Conducting ASPs in the Ambulatory Setting
Compared with the inpatient setting, there is limited guidance available for ASP teams to develop and implement an outpatient ASP service, and it is crucial to identify targets that are critical for program success yet feasible in the distinct outpatient setting.14 The first steps in creating an ambulatory ASP are to define a practice community, identify key stakeholders, build the outpatient ASP team, and establish clear goals and objectives for the program.15 Differing from an inpatient ASP model, core members of the ambulatory ASP team may be involved in direct patient care to a lesser extent and more responsible for creating, implementing, and assessing practice initiatives, education, and monitoring antimicrobial use and resistance patterns of the organisms.15 Common ASP initiatives that have demonstrated success in the ambulatory setting include clinical decision support tools, provider and patient education, evidence-based guidelines, communication training for providers, and delayed prescribing strategies.14,22
Related Content



When employing new ASP initiatives in any setting, local stewards should conduct an evidence-based appraisal of antimicrobial prescribing for various infectious disease syndromes and provider groups to identify barriers to optimal management.12,14,15 It is then crucial to prioritize interventions to target resources and education to areas where there will likely be the most impact.12,14,15 First, evaluate your local data, assess which antimicrobial prescribing issues lie within your institution or health system, and focus your efforts on high-level options.
Stenehjem and colleagues conducted a large retrospective cohort study of urgent care encounters over a 23-month period with the primary objective of characterizing antibiotic prescribing and potential prescribing variability across urgent care visits.23 Following a review of 1.16 million urgent care encounters, antibiotics were prescribed in more than 30% of all encounters, with the rates of antibiotic prescribing being highest for respiratory conditions (61.1%), followed by genitourinary conditions (18.0%) and skin and soft tissue infections (13.9%). Furthermore, 50% of all respiratory encounters resulted in antibiotic prescriptions, yet there was drastic variability at the clinic and provider level, with clinic and provider prescribing variability ranging from 31% to 84% and from 3% to 94%, respectively.23
One could begin to target ambulatory ASP efforts through engaging with higher-volume antimicrobial prescribers (eg, top 10% of providers, specialty groups, or clinics who prescribe antimicrobials).12,14,15 Of note, CDC data have shown that the highest 10% of antibiotic prescribers are responsible for more than 40% of all antibiotic prescriptions in certain populations.24 Another effort could be aimed at targeting the top 1 to 3 indications in which ambulatory antimicrobials are prescribed.12 A common ASP intervention in the ambulatory setting is to reduce inappropriate antibiotic prescribing for uncomplicated respiratory tract infections (RTIs), as this is an obvious target given the well-documented overuse of antibiotics for these infectious syndromes that are primarily viral in nature.14,25
Another concept that is crucial to the success of any ASP initiative is a comprehensive education plan for clinicians.14 Given that the clinician audience is likely to be dispersed across various clinics, pharmacies, and other locations, the educational methods selected for use should be mixed (eg, didactic presentations [virtual likely most effective], posters, brochures, electronic medical record alerts, smartphone apps).14 As such, Gonzales and colleagues aimed to reduce antibiotic use for uncomplicated RTIs through a prospective pre- versus post-analysis in 4 primary care practices.26 The full intervention site used various educational materials, including “academic detailing” (an organized educational program that provides clinicians with evidence-based care to improve patient outcomes) while control sites provided usual care. After the intervention, there was a significant reduction in antibiotic prescribing from 74% to 48%, with no meaningful reductions seen in the control arm.26
Patient education also has been shown to be an effective method for outpatient ASP efforts; a significant driver of unnecessary prescribing has been the expectation of patients to obtain antimicrobials.12,14,15,27
A simple patient educational tool includes symptomatic management “prescription” pads, which target the outpatient management of infections that are commonly viral in origin.12 The primary purpose of resources such as these is to allow providers a convenient resource to provide tangible and tailored recommendations to patients for symptomatic relief of various symptoms that may not require antibiotic prescriptions, as they are likely viral in nature (eg, nasal congestion). Furthermore, these pads also may provide the justification against antibiotic use for illnesses caused by viruses, outline nonpharmacologic methods that can augment symptomatic relief, and provide instructions for provider follow-up if symptoms fail to resolve or worsen. One example of a “Viral Rx Pad” can be found in the review conducted by Jensen and colleagues.12
In addition, patient education also can occur in ways as simple as hanging educational fliers detailing appropriate antibiotic use in various clinics and community pharmacists (eg, “4 Facts for Sinusitis Management”). Provider discussions with patients and caregivers in tandem with educational materials may decrease the expectations of patients and caregivers to receive prescriptions for infections that are typically self-limiting, and these strategies could reduce pressure on providers to write antibiotic prescriptions on patient demand.12
Despite the previously described, individual components being important for ASP efforts, a multifaceted approach for conducting ASP in the outpatient setting is likely most effective. These efforts may include, but are not limited to, provider and patient education, prescriber feedback and “peer comparison reporting,” outpatient ASP dashboards that display antibiotic use metrics, and pre-populated ambulatory order panels.12,14,15 Leveraging technology and the electronic health record are invaluable tools for ambulatory ASP efforts and busy outpatient providers, and they can provide an opportunity to support ASP efforts at the time of prescribing.14 Specifically, syndrome-based, pre-populated order panels may provide an avenue to communicate indirectly to providers by focusing on the differentiation of commonly encountered outpatient respiratory infection diagnoses (eg, sinusitis, bronchitis, community-acquired pneumonia, etc). If a diagnosis was selected by a provider that was commonly viral (ie, sinusitis), the order set may implement cascading logic that drives prescribing efforts to be focused on supportive care, rather than prescriptions for antibiotics. Conversely, a true bacterial infection necessitating an antibiotic prescription could have cascading logic to guide the selection of antibiotic, dose, and duration.12,14,15
One study conducted by Ilges and colleagues was a quasi-experimental, retrospective cohort of all outpatient encounters with a tier 3 (“never prescribe”) upper RTI diagnosis that evaluated this approach.28 The primary objective of this study was to evaluate the frequency of unnecessary antibiotic prescribing pre- and post-implementation of a multifaceted outpatient ASP bundle, including a pre-populated ambulatory order panel. After evaluation of more than 165,000 tier 3 encounters (58.0% pre-implementation, vs 42.0% post-implementation), implementation of the ASP bundle was associated with lower antibiotic prescribing (21.7% vs 11.2%; P<0.001).28
Conclusion
AMR is rising at devastating rates and contributes substantially to morbidity and mortality throughout the world.1 In hopes of mitigating rising rates of AMR, ASPs have emerged to track, report, educate on, and optimize antimicrobial use.6 Despite many successful inpatient ASPs that have been established for decades, there is a substantial lack of formal outpatient ASPs throughout the United States, which may be due to a shortage of dedicated resources and distinct differences in treatment settings.11,12 Optimizing antimicrobial use throughout all treatment settings should be the standard of care, and the development and implementation of universal ambulatory ASP efforts should be a national and international priority. Given the various strategies and techniques in which ASP efforts can be successfully conducted throughout ambulatory settings, it is important to highlight the numerous available resources and bundles to assist with outpatient ASP efforts, including those from the CDC and Society of Infectious Diseases Pharmacists.12,14,15,21,29
References
- Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629-655.
- WHO. Antimicrobial resistance. November 21, 2023. Accessed November 22, 2024. https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance
- CDC. Antibiotic Resistance Threats in the United States, 2019. Department of Health and Human Services, CDC; 2019. Accessed November 22, 2024. https://www.cdc.gov/antimicrobial-resistance/media/pdfs/2019-ar-threats-report-508.pdf
- CDC. Antibiotic Resistance Threats in the United States, 2013. Department of Health and Human Services, CDC; 2013. Accessed November 22, 2024. https://www.cdc.gov/antimicrobial-resistance/media/pdfs/ar-threats-2013-508.pdf
- Tang KWK, Millar BC, Moore JE. Antimicrobial resistance (AMR). Br J Biomed Sci. 2023;80:11387.
- Fishman N. Policy statement on antimicrobial stewardship by the Society for Healthcare Epidemiology of America (SHEA), the Infectious Diseases Society of America (IDSA), and the Pediatric Infectious Diseases Society (PIDS). Infect Control Hosp Epidemiol. 2012;33(4):322-327.
- Dyar OJ, Huttner B, Schouten J, et al. What is antimicrobial stewardship? Clin Microbiol Infect. 2017;23(11):793-798.
- CDC. Core Elements of Hospital Antibiotic Stewardship Programs. Department of Health and Human Services, CDC; 2019. Accessed November 22, 2024. https://www.cdc.gov/antibiotic-use/healthcare/pdfs/hospital-core-elements-H.pdf
- CDC. Antibiotic use and stewardship in the United States, 2023 update: progress and opportunities. April 22, 2024. Accessed November 22, 2024. https://www.cdc.gov/antibiotic-use/hcp/data-research/stewardship-report.html
- CDC. Outpatient antibiotic prescribing in the United States. April 22, 2024. Accessed November 22, 2024. https://www.cdc.gov/antibiotic-use/hcp/data-research/antibiotic-prescribing.html?CDC_AAref_Val=//www.cdc.gov/antibiotic-use/data/outpatient-prescribing/index.html
- Eudy JL, Pallotta AM, Neuner EA, et al. Antimicrobial stewardship practice in the ambulatory setting from a national cohort. Open Forum Infect Dis. 2020;7(111):ofaa513.
- Jensen KL, Rivera CG, Draper EW, et al. From concept to reality: building an ambulatory antimicrobial stewardship program. JACCP. 2021;4(12):1583-1593.
- Hersh AL, King LM, Shapiro DJ, at el. Unnecessary antibiotic prescribing in US ambulatory care settings, 2010-2015. Clin Infect Dis. 2021;72(1):133-137.
- Dobson EL, Klepser ME, Pogue JM, et al. Outpatient antibiotic stewardship: interventions and opportunities. J Am Pharm Assoc (2003). 2017;57(4):464-473.
- Klepser ME, Dobson EL, Pogue JM, et al. A call to action for outpatient antibiotic stewardship. J Am Pharm Assoc (2003). 2017;57(4):457-463.
- CDC. Outpatient antibiotic prescriptions— United States, 2022. Last reviewed November 15, 2023; Accessed October 30, 2024. https://archive.cdc.gov/#/details?url=//www.cdc.gov/antibiotic-use/data/report-2022.html
- Jones BE, Sauer B, Jones MM, et al. Variation in outpatient antibiotic prescribing for acute respiratory infections in the veteran population: a cross-sectional study. Ann Intern Med. 2015;163(2):73-80.
- Van Duin D, Paterson DL. Multidrug resistant bacteria in the community: an update. Infect Dis Clin North Am. 2020;34(4):709-722.
- Saravolatz LD, Pohlod DJ, Arking LM. Community-acquired methicillin-resistant Staphylococcus aureus infections: a new source for nosocomial outbreaks. Ann Intern Med. 1982;97(3):325-329.
- The Joint Commission. Antimicrobial stewardship in ambulatory health care. R3 Report. June 20, 2019;23. Accessed November 22, 2024. https://www.jointcommission.org/-/media/tjc/documents/standards/r3-reports/r3_23_antimicrobial_stewardship_amb_6_14_19_final2.pdf
- Sanchez GV, Fleming-Dutra KE, Roberts RM, at el. Core Elements of Outpatient Antibiotic Stewardship. MMWR Morb Mortal Wkly Rep Recomm Rep. 2016;65(No. RR-6):1-12.
- Drekonja DM, Filice GA, Greer N, et al. Antimicrobial stewardship in outpatient settings: a systematic review. Infect Control Hosp Epidemiol. 2015;36(2):142-152.
- Stenehjem E, Wallin A, Fleming-Dutra KE, et al. Antibiotic prescribing variability in a large urgent care network: a target for outpatient stewardship. Clin Infect Dis. 2020;70(8):1781-1787.
- Gouin KA, Fleming-Dutra KE, Tsay S, et al. Identifying higher-volume antibiotic outpatient prescribers using publicly available Medicare Part D data – United States, 2019. MMWR Morb Mortal Wkly Rep. 2022;71(6):202-205.
- Shapiro DJ, Hicks LA, Pavia AT, et al. Antibiotic prescribing for adults in ambulatory care in the USA, 2007-09. J Antimicrob Chemother. 2014;69(1):234-240.
- Gonzales R, Steiner JF, Lum A, et al. Decreasing antibiotic use in ambulatory practice: impact of a multidimensional intervention on the treatment of uncomplicated acute bronchitis in adults. JAMA. 1999;281(16):1512-1519.
- Kohut MR, Keller SC, Linder JA, et al. The inconvincible patient: how clinicians perceive demand for antibiotics in the outpatient setting. Fam Pract. 2020;37(2):276-282.
- Ilges D, Jensen K, Draper E, et al. Evaluation of multisite programmatic bundle to reduce unnecessary antibiotic prescribing for respiratory infections: a retrospective cohort study. Open Forum Infect Dis. 2023;10(12):ofad585.
- CDC. Antibiotic stewardship resource bundles. April 23, 2024. Accessed November 22, 2024. https://www.cdc.gov/antibiotic-use/hcp/educational-resources/stewardship/index.html
About the authors:


Dr. Gruss reported no relevant financial disclosures. Dr. Morrisette receives grant funding through AbbVie and Stellus Rx; has participated in scientific advisory boards for AbbVie and Basilea Pharmaceutica; has provided expert witness testimony to Copeland Stair Valz & Lovell; and has received honoraria from IDSE.
Copyright © 2024 McMahon Publishing, 545 West 45th Street, New York, NY 10036. Printed in the USA. All rights reserved, including the right of reproduction, in whole or in part, in any form.

Download to read this article in PDF document:![]() Outpatient Antimicrobial Stewardship: A Road Less Traveled
Outpatient Antimicrobial Stewardship: A Road Less Traveled