


In the summer of 1981, the CDC released a Morbidity and Mortality Weekly Report that described Pneumocystis carinii pneumonia, a rare condition, in five previously healthy young males in Los Angeles. This publication marked the first official report of what came to be known as the AIDS epidemic.1 HIV, the cause of AIDS, primarily targets and destroys CD4+ T cells, with CD4+ T-cell measurement being a common method to categorize the progression of disease and level of immunosuppression.2
Lower CD4+ T-cells lead to a higher risk for developing opportunistic infections (OIs), which are infections due to organisms that do not normally cause disease but become pathogenic when an individual’s immune system is impaired. Furthermore, OIs can be classified as illnesses that are more severe and occur more frequently in people who are immunosuppressed.3,4 Although the development and implementation of antiretroviral therapy has dramatically reduced the incidence of OIs, they still remain the main driver of morbidity and mortality in people living with HIV/AIDS. Therefore, medication adherence is essential.5-7
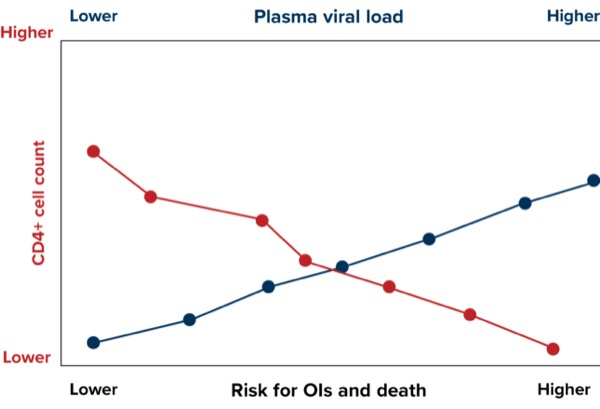
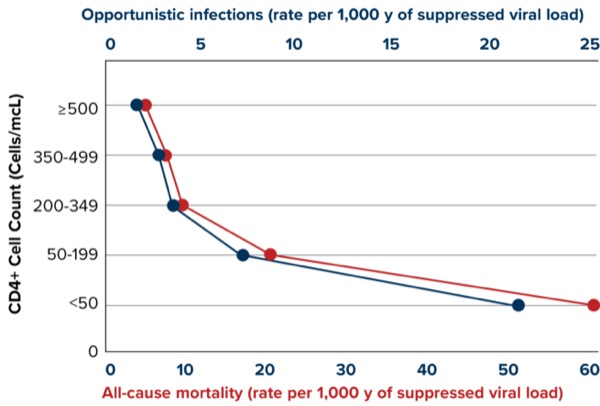
HIV is estimated to be diagnosed in nearly 40 million people worldwide, which underscores the importance of early diagnosis and treatment of OIs to improve patient outcomes.8 A greater CD4+ cell count and a lower plasma viral load are associated with a lower risk of OIs and death9 (Figures 1 and 2).
Most of the evidence regarding OIs in people with HIV/AIDS focuses primarily on fungi and viruses, while bacterial OIs are often overlooked and neglected by the HIV community.10 Important work conducted by O’Connor and colleagues contributed new evidence that severe bacterial infections other than those caused by Mycobacterium tuberculosis should be recognized as HIV-related opportunistic infections.11 In this report, bacterial pneumonia, skin and soft tissue infections, and urinary tract infections (UTIs) accounted for nearly 70% of non-tuberculosis severe bacterial events in their cohort of nearly 5,000 patients.11
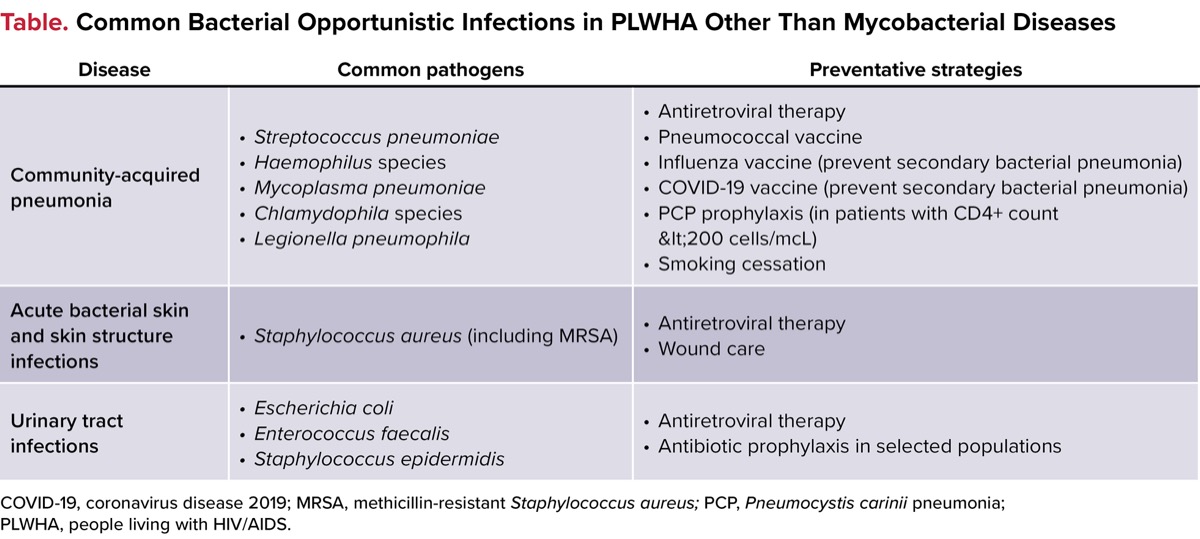
The common pathogens and preventative strategies for bacterial pneumonia, acute bacterial skin and skin structure infections (ABSSSIs), and UTIs are shown in the Table.12 The purpose of this review is to discuss bacterial OIs and antibiotic use in people with HIV/AIDS, excluding mycobacterial disease.
| Table. Common Bacterial Opportunistic Infections in PLWHA Other Than Mycobacterial Diseases | ||
| Disease | Common pathogens | Preventative strategies |
|---|---|---|
| Community-acquired pneumonia |
|
|
| Acute bacterial skin and skin structure infections |
|
|
| Urinary tract infections |
|
|
| COVID-19, coronavirus disease 2019; MRSA, methicillin-resistant Staphylococcus aureus; PCP, Pneumocystis carinii pneumonia; PLWHA, people living with HIV/AIDS. | ||
Pneumonia
Pneumonia has been reported to be the second most common cause of hospitalizations and the leading cause of infection-related deaths in the United States.13,14 Furthermore, despite substantial advances in treatment, bacterial respiratory diseases and pneumonia lead to a high level of morbidity in people with HIV/AIDS, especially in patient populations who have poor access to medical care.15-18 Pneumocystis jirovecii and M. tuberculosis are typically the emphasized pathogens when discussing AIDS-associated respiratory diseases; however, other bacteria can be associated with a high incidence of pneumonia.11,19
Figueiredo-Mello and colleagues conducted an etiologic investigation of community-acquired respiratory infections in 224 people with HIV/AIDS, with a cause being determined among 143 (64%).20 Among the non-TB bacterial diseases, 15% of cases were due to Streptococcus pneumoniae, while Mycoplasma pneumoniae and Chlamydophila pneumoniae were identified in 8% and 5%, respectively.20 Importantly, the risk for invasive S. pneumoniae disease is higher in people with HIV/AIDS than the general population.21
Of note, community-acquired and hospital-acquired/ventilator-associated pneumonia guidelines do not focus on patients with immunocompromising conditions. In general, the basic principles of treatment for confirmed bacterial pneumonia in people with HIV/AIDS are similar to treating those without HIV/AIDS. These pneumonias can occur at any CD4+ T-cell count.12,22-24
Furthermore, a matched case-control evaluation conducted by Christensen and colleagues indicated that clinical outcomes of patients hospitalized with community-acquired pneumonia were not influenced by the presence of HIV infection.25 However, it is crucial for clinicians to consider previous antibiotic prophylaxis, and the clinical presentation should strongly suggest non–M. tuberculosis disease prior to initiating fluoroquinolone therapy, because fluoroquinolone monotherapy could lead to fluoroquinolone resistance in patients with active tuberculosis.26
Acute Bacterial Skin and Skin Structure Infections
ABSSSIs are a common cause of primary care and/or emergency department visits in the United States.27,28 Importantly, people with HIV/AIDS have an increased risk for ABSSSIs, including those caused by methicillin-resistant Staphylococcus aureus.29,30
Hemmige and colleagues sought to determine the epidemiological and microbiological characteristics of ABSSSIs in people with HIV in a large, urban country health system.31 Over a 5-year period, they identified more than 2,200 ABSSSIs, with 22.8% associated with culture data. Of these cultured ABSSSIs, 66.0% included S. aureus as at least 1 organism, of which 86.4% featured S. aureus in monomicrobial infections. Most of these infections were methicillin-resistant (69.8%).31
Related Content


Importantly, people who inject drugs are also at an increased risk for both HIV and ABSSSIs.32,33 In fact, 10% of all HIV diagnoses in 2018 were attributed to practices associated with unsafe injection drug use or male-to-male sexual contact among people who inject drugs.34 The mechanisms between injection drug use and subsequent development of HIV include the process of sharing syringes, needles, and/or other equipment that someone with HIV has used.33
Although the exact mechanisms for the development of ABSSSIs in people who inject drugs are not fully elucidated, they include contaminated needles coupled with a disrupted cutaneous barrier, microvascular damage, local tissue injury, venous thrombosis, and impaired venous and lymphatic drainage because of frequent and repeated non-sterile injection.35 Approaches that reduce the frequency of injection drug use, utilization of contaminated equipment, needle/syringe/equipment sharing, and various other high-risk behaviors may be effective in preventing both HIV and ABSSSIs in people who inject drugs.35
Generally, the treatment of people living with HIV/AIDS with ABSSSIs should be based on pathogens and phenotypes isolated (if applicable) or common organisms that are responsible for the various subtypes of skin infections (cellulitis, abscesses, and others).36 Importantly, other risk factors associated with the development of ABSSSIs in people with HIV have included diabetes, psoriasis, lymphedema, the presence of an intravenous catheter, and antibiotic use.29,37 Specifically, Crum-Cianflone and colleagues evaluated ABSSSIs in a prospective cohort of more than 1,900 people living with HIV and evaluated antibiotic use by specific class in separate multivariable models. They found that tetracycline, macrolide, fluoroquinolone, and beta-lactam use within the previous 12 months was associated with a significantly increased risk for initial ABSSSIs.29
Urinary Tract Infections
UTIs are among the most frequent infections for which antibiotics are prescribed in adults in the United States, and are a common cause of morbidity and antibiotic use in people with HIV/AIDS.38 However, UTIs remain an underinvestigated clinical problem in people with HIV/AIDS. Furthermore, many of the studies assessing UTIs and antibiotic use in people with HIV/AIDS have been conducted outside the United States.39-41 Birhanu and colleagues conducted a systematic review and meta-analysis that evaluated the magnitude of UTIs among people living with HIV in Ethiopia. Of 7 studies that included nearly 2,300 subjects, the overall prevalence was 12.8%.39
Skrzat-Klapaczynska and colleagues evaluated factors associated with the occurrence of UTIs in people with HIV/AIDS from outpatient clinics in Poland. The most frequently isolated pathogens were Escherichia coli (58.2%), followed by Enterococcus faecalis (12.8%) and Staphylococcus epidermidis (5.0%). Multivariable logistic regression suggested that being female and heterosexual coital acts increased the odds of infection, while higher nadir CD4+ T-cell count decreased the odds of UTIs.40 Another study, this one a cross-sectional analysis, was conducted in people with HIV/AIDS with UTIs caused by E. coli. They also found high-resistance rates to ampicillin, ceftriaxone, ciprofloxacin, and cotrimoxazole.41
Novel Antimicrobials
Novel antimicrobials are needed to combat the continuous increase in bacterial resistance.42 Of note, studies report a very low prevalence of novel antibiotic use in people with HIV/AIDS. In prospective clinical research, people with HIV/AIDS may be excluded from trials that evaluate novel antibiotics for the treatment of many infections, since clinicians may believe that HIV/AIDS will confound an appropriate evaluation of outcomes. Because this information is important to clinicians that treat people with HIV/AIDS, additional research is warranted to investigate the efficacy of antibiotics in people with HIV/AIDS.25
Conclusion
Although the life span of people with HIV/AIDS has increased dramatically following the development and implementation of antiretroviral therapy, lifelong medication adherence is imperative to maintain good health outcomes.5 In patients with reduced CD4+ T-cell counts, OIs lead to a high degree of morbidity and mortality in people with HIV/AIDS.6,7 Of the non-TB bacterial causes of OIs, other bacterial pneumonias, ABSSSIs, and UTIs are prevalent in the HIV/AIDS population.
Real-world observational data are emerging with many novel antimicrobials that provide favorable evidence for the use of these medications in many indications.43,44 Despite the promise of these novel agents, few studies include a high prevalence of the use of these antibiotics in people with HIV/AIDS. Further research of traditional and novel antibiotics should include people with HIV/AIDS to evaluate the effectiveness of these agents in this patient population.
References
- Centers for Disease Control and Prevention (CDC). MMWR Morb Mortal Wkly Rep. 1981;30(21):1-3.
- Battistini Garcia SA, Guzman N. StatPearls [Internet]. StatPearls Publishing; 2023.
- Centers for Disease Control and Prevention (CDC). Accessed April 13, 2024. https://www.cdc.gov/hiv/basics/livingwithhiv/opportunisticinfections.html
- Zaremba ML. Przegl Epidemiol. 2001;55 suppl 3:91-99.
- Palmisano L, Vella S. Ann Ist Super Sanita. 2011;47(1):44-48.
- Djawe K, Buchacz K, Hsu L, et al. J Infect Dis. 2015;212(9):1366-1375.
- Meng S, Tang Q, Xie Z, et al. Eur J Clin Microbiol Dis. 2023;42(1):113-120.
- World Health Organization. HIV. Accessed April 20, 2024. https://www.who.int/data/gho/data/themes/hiv-aids
- Young J, Psichogiou M, Meyer L, et al. PLoS Med. 2012;9(3):e1001194.
- Anglaret X, Eholie SP. Lancet HIV. 2017;4(3):e94-e95.
- O’Connor J, Vjecha MJ, Phillips AN, et al. Lancet HIV. 2017;4(3):e105-e112.
- US Department of Health and Human Services. Panel on Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV. Accessed April 24, 2024. https://clinicalinfo.hiv.gov/sites/default/files/guidelines/documents/adult-adolescent-oi/guidelines-adult-adolescent-oi.pdf
- Pfunter A, Wier LM, Stocks C. Most frequent conditions in U.S. hospitals, 2011. HCUP Statistical Brief #162, Agency for Healthcare Research and Quality. September 2013.
- Xu J, Murphy SL, Kochanek KD, et al. Natl Vital Stat Rep. 2016;64(2):1-119.
- Caiaffa WT, Graham NM, Vlahov D. Am J Epidemiol. 1993;138(11):909-922.
- Segal LN, Methé BA, Nolan A, et al. Proc Am Thorac Soc. 2011;8(3):282-227.
- Schwarcz S, Hsu L, Dilley JW, et al. J Acquir Immune Defic Syndr. 2006;43(4):491-494.
- Grau I, Pallares R, Tubau F, et al. Arch Intern Med. 2005;165(13):1533-1540.
- Davis JL, Fei M, Huang L. Curr Opin Infect Dis. 2008;21(2):184-190.
- Figueiredo-Mello C, Naucler P, Negra MD, et al. Medicine (Baltimore). 2017;96(4):e5778.
- Kyaw MH, Rose CE Jr, Fry AM, et al. J Infect Dis. 2005;192(3):377-386.
- Metlay JP, Waterer GW, Long AC, et al. Am J Respir Crit Care Med. 2019;200(7):e45.
- Kalil AC, Metersky ML, Klompas M, et al. Clin Infect Dis. 2016;63(5):e61-e111.
- Huang L, Crothers KA. Respirology. 2009;14(4):474-485.
- Christensen D, Feldman C, Rossi P, et al. Clin Infect Dis. 2005;41(4):554-556.
- Ginsburg AS, Hooper N, Parrish N, et al. Clin Infect Dis. 2003;37(11):1448-1452.
- Hersh AL, Chambers HF, Maselli JH, et al. Arch Intern Med. 2008;168(14):1585-1591.
- Cairns C, Kang K. Accessed May 2. https://www.cdc.gov/nchs/data/nhamcs/web_tables/2021-nhamcs-ed-web-tables-508.pdf
- Crum-Cianflone NF, Grandits G, Weintrob A, et al. Int J STD AIDS. 2012;23(7):507-511.
- Popovich KJ, Weinstein RA, Aroutcheva A, et al. Clin Infect Dis. 2010;50(7):979-987.
- Hemmige V, Arias CA, Pasalar S, et al. Clin Infect Dis. 2020;70(9):1985-1992.
- Hemmige V, McNulty M, Silverman E. BMC Infect Dis. 2015;15:455.
- Centers for Disease Control and Prevention. HIV surveillance report: diagnoses of HIV infection in the United States and dependent areas, 2018 (updated). 2020.
- CDC. HIV Surveillance Report, 2019; vol 32. Published May 2021. Accessed June 2024. https://www.cdc.gov/hiv/pdf/library/reports/surveillance/cdc-hiv-surveillance-report-2018-updated-vol-32.pdf.
- Chambers HF. Infect Dis Clin North Am. 2021;35(1):169-81.
- Stevens DL, Bisno AL, Chambers HF, et al. Clin Infect Dis. 2014;59(2):e10-52.
- Hemmige V, McNulty M, Silverman E, et al. Eur J Clin Microbiol Infect Dis. 2015;34(2):339.
- Hersh AL, King LM, Shapiro DJ, et al. Clin Infect Dis. 72(1):133-137.
- Birhanu MY, Habtegiorgis SD, Gietaneh W, et al. PLoS One. 2022;17(4):e0264732.
- Skrzat-Klapaczynska A, Matlosz B, Bednarska A, et al. PLoS One. 2018;13(1):e0190564.
- Abongomera G, Koller M, Musaazi J, et al. BMJ Infect Dis. 2021;21(1):1179.
- Salam MA, Al-Amin MY, Salam MT, et al. Healthcare (Basel). 2023;11(13):1946.
- Lodise TP, Gunter K, Mu F, et al. J Manag Spec Pharm. 2023;29(8):952-964.
- Kunz Coyne AJ, Alosaimy S, Lucas K, et al. Microbiol Spectr. 2024;12(1):e0235123.
About the authors:


Copyright © 2024 McMahon Publishing, 545 West 45th Street, New York, NY 10036. Printed in the USA. All rights reserved, including the right of reproduction, in whole or in part, in any form.

Download to read this article in PDF document:![]() Bacterial Infections and Antibiotic Use In People Living With HIV/AIDS
Bacterial Infections and Antibiotic Use In People Living With HIV/AIDS