


Maintain a high degree of suspicion for histoplasmosis in the immunocompromised host, especially if they live in the “Histo Belt,” experts warned.
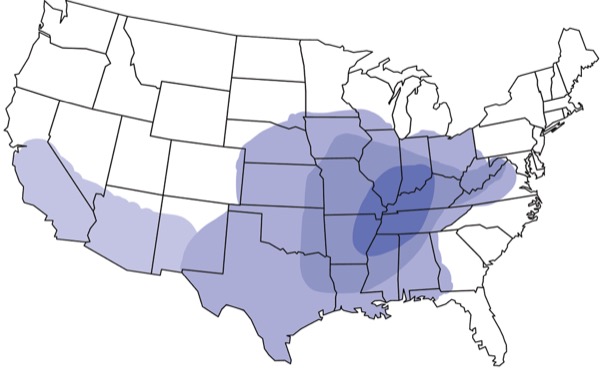
Disseminated histoplasmosis is an invasive fungal infection that may infect the immunocompromised, including those with HIV, in certain parts of the United States, most commonly the Ohio and Mississippi River valleys. In these “Histo Belt” geographic areas, soil and bat or bird droppings may harbor the fungal culprit.
“This is something we are breathing literally every single day,” said Chinelo Animalu, MD, MPH, FACP, FIDSA, the lead author of two cases and a review of combined antifungal and steroid therapy (Case Rep Infect Dis 2025;2025:2623694).
In patients with HIV, widespread infection involves multiple body systems—such as the lungs, bone marrow and skin—said Dr. Animalu, an associate professor in the Division of Infectious Diseases at the University of Tennessee Health Science Center, in Memphis. Hemophagocytosis can occur in the setting of certain infections, such as histoplasmosis, and it can be fatal if not diagnosed early.
“Given that the three disease entities involved including AIDS, disseminated histoplasmosis and hemophagocytosis can all present with nonspecific symptoms and febrile pancytopenia, this can lead to delayed diagnosis and subsequent poorer outcomes,” the researchers noted in the case reports. “Due to the rarity of this combination, the best treatment for histoplasmosis complicated by hemophagocytosis remains uncertain and can vary from patient to patient.”
The researchers described two cases of U.S. patients with uncontrolled HIV and a history of nonadherence to antiretroviral therapy who presented with disseminated histoplasmosis with persistent febrile pancytopenia, which was found to be hemophagocytosis. In each case, the patient received antifungals and underwent a bone marrow biopsy to determine a diagnosis of hemophagocytosis. Their fever resolved and pancytopenia improved with the addition of corticosteroids to antifungal therapy, highlighting the need for a more reliable standard of pharmacologic management, the clinicians said.
Dr. Animalu and her collaborators wrote the paper “to create awareness for our doctors or clinicians who may not know that you could have multiple diseases with similar symptoms,” she explained. Involving an infectious disease physician is paramount.
These cases underscore the possibility of hemophagocytosis among patients with HIV or other immunosuppressive conditions in regions endemic to particular diseases, such as Histoplasma capsulatum, Anaplasma, Ehrlichia or other infectious etiologies and in individuals who remain pancytopenic or do not respond to treatment of the underlying infection. A bone marrow biopsy may be needed to ascertain the existence of underlying hemophagocytosis.
Treat the Underlying Problem, Too
The researchers pointed out that there are no randomized clinical trials supporting definitive treatment of this condition secondary to infectious etiologies. To boost survival, treating these underlying etiologies is important.
“These two cases, plus the literature review, reinforce a practical point: When antifungal treatment alone isn’t enough and the patient’s counts keep falling, adding steroids can be the difference between recovery and decline,” said Jake Scott, MD, a clinical associate professor specializing in infectious diseases and geographic medicine at Stanford Medicine, in Palo Alto, Calif. He was not involved in the case reports.
Related Content

In patients with advanced HIV and living in—or recently traveling through—histoplasmosis endemic regions, physicians should be vigilant for hemophagocytosis amid fever and low blood counts. He recommended promptly starting amphotericin B. If fever and pancytopenia persist after about 72 hours, he advised to check ferritin levels and consider a bone marrow biopsy. And if hemophagocytosis seems probable, he would prescribe dexamethasone while continuing antifungal treatment. Early dual therapy can be lifesaving, whereas delays can result in poor outcomes.
“Prospective studies comparing amphotericin alone versus amphotericin plus steroids would help refine future guidance,” Dr. Scott said. “Meanwhile, the pragmatic lesson is clear: Treat the fungus quickly, monitor the labs closely and don’t hesitate to quiet the immune system when hemophagocytosis is suspected.”
Amid increasing reports of hemophagocytosis with histoplasmosis in the last few years, clinicians are interested in determining whether targeted therapies provide an added benefit to antifungal treatment, said Zachary Mostel, MD, AAHIVS, a fellow in the Division of Infectious Diseases at the Icahn School of Medicine at Mount Sinai, in New York City.
Dr. Mostel advises maintaining “a high degree of suspicion for hemophagocystosis and histoplasmosis in the immunocompromised host,” he said. “These entities are both mimickers of many other infectious, inflammatory and malignant diseases. The potential benefit of these agents must be weighed against the risk of further bone marrow suppression, which can cause bleeding and other opportunistic infections.”
A large clinical trial assessing the benefit of hemophagocytosis-directed therapies remains unlikely, so “my hope is that ongoing reporting of successful cases will contribute to a stronger evidence base, ultimately informing future practice guidelines and improving patient outcomes,” Dr. Mostel said.
Drs. Animalu, Mostel and Scott reported no relevant financial disclosures.
This article is from the June 2025 print issue.