

Because of defunding threats, HIV research and programs in the United States may be retired to the halls of history. Scientists and epidemiologists in health agencies like the CDC have been fired, although a fraction were rehired. Departments are being closed or consolidated with little notice. Grant funding is being delayed or canceled, and some universities, in particular, have been targeted. All these actions have caused chaos, leaving some HIV researchers to rethink their careers.
“The NIH research cuts are forcing some in HIV research to consider alternative career pathways,” said Steven G. Deeks, MD, a professor of medicine in residence at the University of California, San Francisco (UCSF), and a faculty member at Zuckerberg San Francisco General Hospital.
Funding for young investigators also has been decreased, which threatens the future of U.S. research, according to Diane V. Havlir, MD, a professor of medicine at UCSF. “Science depends on a pipeline of young investigators,” said Dr. Havlir, who is also the Robert Weiss Memorial Chair for HIV/AIDS research, director of the UCSF AIDS Research Institute and chief of HIV, Infectious Diseases and Global Medicine at Zuckerberg Hospital.
“The biggest problems in science can be solved by bringing experienced and young investigators together, and [the administration’s actions] will impact on people’s interest in going into science—not just HIV.

“If no funding is coming in, people who have laboratories, people who have ongoing studies can’t pay their staff and keep the programs running,” Dr. Havlir said.
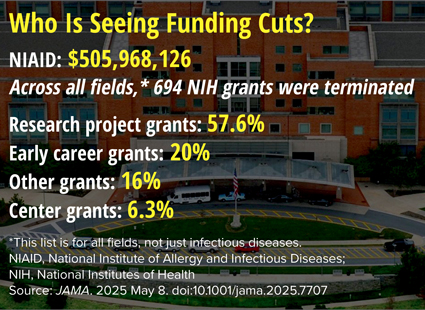
The Trump administration has said repeatedly that the cuts are aimed at “rooting out waste,” a message that is reinforced in the FY2026 Department of Health and Human Services (HHS) budget.
Grant funding for research that appears to violate executive orders also has been halted, most notably involving transgender people, even though 1 million Americans identify as transgender, and they comprised about 2% of new HIV diagnoses a year in this country, according to the CDC (bit.ly/3ZnmWxJ-IDSE). “That is an example of an outsized impact on HIV research,” Dr. Havlir said. (A quick search on ClinicalTrials.gov found more than 100 studies involved HIV and transgender people.)

Axing HIV Vaccine Research
Just days before Infectious Disease Special Edition went to press, the administration defunded two HIV vaccine research programs at the Duke Human Vaccine Institute and the Scripps Research Institute because the administration said current prevention programs are sufficient—even though 38,000 new HIV infections are diagnosed each year in the United States alone, according to CDC data (MMWR Morb Mortal Wkly Rep 2019;68[48]:117-123). The Moderna HIV vaccine study also was on the chopping block.
This defunding comes as Australian researchers published a paper on using mRNA technology to eradicate latent HIV by activating viral transcription to cure this disease (Nat Commun 2025;16[1]:4979).
“This [defunding] represents an enormous setback for the development of a vaccine against the virus that causes AIDS,” Duke officials told Infectious Disease Special Edition in an email. “In the more than two decades since the Duke Human Vaccine Institute received the initial seven-year grant from the National Institute of Allergy and Infectious Diseases, CHAVD [Center for HIV/AIDS Vaccine Development] researchers at Duke and affiliated institutions around the country have not only made significant discoveries about HIV, but have also contributed to the science that has led to a new pan-coronavirus vaccine and autoimmune therapies.”
When asked about the cuts, an HHS spokesperson said the FY2026 HHS budget would eliminate “duplication of efforts,” but assured that “critical HIV/AIDS programs will continue under the Administration for a Healthy America (AHA),” a new HHS department. HHS Secretary Robert F. Kennedy Jr.’s budget brief noted that the FY2024 budget had allocated $7.5 billion to 27 separate programs that addressed HIV/AIDS, which he decided were “wasteful and inefficient.”
This is a far cry from the Feb. 5, 2019, State of the Union address, when President Donald Trump committed to ending HIV transmission by 2030. “In recent years we have made remarkable progress in the fight against HIV and AIDS. Scientific breakthroughs have brought a once-distant dream within reach. My budget will ask Democrats and Republicans to make the needed commitment to eliminate the HIV epidemic in the United States within 10 years. Together, we will defeat AIDS in America.”
The FY2026 budget has proposed cuts to HIV, sexually transmitted infections (STIs), hepatitis B and C, as well as other infectious disease programs and research. These cuts include slashing $74 million from the Ryan White HIV/AIDS Program and cutting $77 million from and consolidating CDC HIV, STI, hepatitis and other programs. “At a time when our country is experiencing rising STI rates, surges in viral hepatitis and persistent health disparities in HIV, cutting these essential programs is reckless,” said Joe Huang-Racalto, the director of Strategic Partnerships and Policy at NMAC, formerly the National Minority AIDS Council. “It is not fiscally responsible to dismantle the infrastructure that keeps people healthy and alive.”
In the 1980s, a person lived about three years after an HIV/AIDS diagnosis. Today the 1.2 million people living with HIV in the United States can expect to live almost as long as someone without the disease, thanks in large part to research funded by the HHS, according to the CDC (bit.ly/3Zl8ZAt-IDSE).
But this research is in peril. “We are seeing delays in getting new grants submitted and reviewed, and finance updates for existing grants [are also delayed],” explained Dr. Deeks, who is also the principal investigator of the Delaney AIDS Research Enterprise and the amfAR Institute of HIV Cure Research. With future funding in limbo, “we are highly constrained at what we can do. So, some of the science is being paused, layoffs are being considered, and it’s having a dramatic effect on our ability to do science.”
Carlos del Rio, MD, the Cliff H. Sauls Distinguished professor of medicine, chair of the Department of Medicine at Emory School of Medicine, as well as the co-director of the Emory Center for AIDS Research and co–principal investigator of the Emory Vaccine and Treatment Evaluation Unit, in Atlanta, said the cuts to HIV prevention, care, treatment and research would have a “tremendous impact” both here and abroad.
Research in HIV has achieved several key milestones, Dr. del Rio stressed, including turning a uniformly fatal infection into a chronic condition, reducing the impact of AIDS here and abroad, and improving America’s standing around the world. But less well known is how HIV research has helped advance the development of treatments for other diseases.
Reducing those funding commitments could have collateral effects for many other fields of medicine, including cancer and autoimmune diseases.
From the Bench to the Bedside
When he was in medical school, Richard E. Chaisson, MD, a professor of epidemiology at the Johns Hopkins School of Medicine, in Baltimore, said he was taught “that if you can treat a bacterium, you can treat a fungus—barely—but you cannot treat a virus.”
But work spearheaded in virology “led to a cascade of drugs being developed for viruses that previously no one thought was possible,” Dr. Chaisson said, including zidovudine, the first successful HIV medication. Even today, AZT still has an important use in HIV management—it is a cornerstone for preventing maternal–fetal transmission.
“Now we have at least 25 drugs for HIV in multiple classes, and we’ve gone from toxic cocktails of the 1990s to one pill a day or one shot every few months.”
That bench science also led to treatments for hepatitis B and a cure for hepatitis C, with the latter “a direct outcome of the virology that was done for HIV,” said Dr. Chaisson, who is also the director of the Johns Hopkins University Center for Tuberculosis Research and the principal investigator of the university's Center for AIDS Research.
HIV studies on the immune system “have implications for transplantation, autoimmune diseases like arthritis, rheumatoid arthritis, lupus, Sjogren’s syndrome and inflammatory bowel disease,” he said, adding that “all of that medicine evolved out of [the study of] HIV.”
HIV Research Yields a Cure for Cancer
Like HIV, the road to curing cancer has been long and arduous, but ideas used in HIV research have increased the pathway to a cure for cancer. A case in point is chimeric antigen receptor T-cell (CAR T) therapy, a cutting-edge cancer treatment that uses the patient’s T-cells and immune system to cause apoptosis of cancer cells. A meta-analysis documented complete remissions of B-cell malignancies lasting three years or longer in more than half of patients undergoing CAR T-cell therapy, with some remissions of up to nine years and counting (J Clin Oncol 2020;38[32]:3805-3815). These breakthroughs can be traced back to early HIV research—some of which was done in Dr. Deeks’ laboratory.
“Back in the late ’80s, a number of groups began to think about how we could leverage or enhance the capacity of CD+ T-cells to prevent or control disease” after the realization that CD+ T-cells were almost “magical” killers, he said. “Because HIV was so well resourced and because there was a tight connection between academia and industry [in HIV], it became a direct pathway to go from the idea in the lab” to patients. His group conducted the first randomized clinical trial for CAR T in the mid-1990s (Mol Ther 2002;5[6]:788-797).
“It didn’t work for HIV, but everyone that was involved in that work went on to discover this cure for cancer. But it was through HIV that they got there,” Dr. Deeks explained.
Domestic Agenda Also Threatened
Unfortunately, HIV research is not the only area seeing cuts. Domestic programs such as the Ryan White HIV/AIDS Program—which provides critical healthcare and social services—also will be squeezed. The budget moves Ryan White from the Health Resources and Services Administration to the new AHA, and eliminates Ryan White Part F (which provides education and training). The program was started by then-President George H.W. Bush, in 1990, with bipartisan support. Today more than 500,000 people with HIV depend on Ryan White services.
Even the FY2026 budget brief calls Ryan White an essential program in the U.S. response to HIV.
Just as HIV research has had far reaching implications for other medical disciplines, the care of people with HIV through the Ryan White program has become a model for delivering comprehensive medical care to anyone.
This is one of the biggest contributions of the Ryan White program—that it has developed models that care for the whole patient, several sources said. From having a medical home to an oncology patient navigator, more and more programs are adopting the idea of treating the whole patient.
“The Ryan White program has been an incredible innovator. We talk about medical homes; Ryan White was the original medical home,” Dr. del Rio said.
“Ryan White was started to help people without insurance and no recourse to public insurance because they were young—they were not eligible for Medicare, and they were not usually eligible for Medicaid,” Dr. Chaisson explained. “It has had a profound impact for medical care; and it has expanded beyond just medical care, but provides comprehensive care and wraparound services, such as social work, transportation, housing assistance, food assistance.” These programs are facilitated, not necessarily financed by, Ryan White.
When the Ryan White HIV/AIDS program began, many people with HIV were unable to access affordable insurance coverage, said Jeffrey Crowley, MPH, a distinguished scholar and the director of the O’Neill Institute for National and Global Health Law Center for HIV and Infectious Disease Policy at Georgetown University Law Center, in Washington, D.C. Today, the program covers about half of all people with HIV in the United States, about 80% of whom also have insurance coverage. “They need Ryan White because the standard benefits package just does not meet all of their needs, and the program is critical to retaining people in care and supporting viral suppression,” he said.
Most of the money for Ryan White is allocated to states and heavily affected metropolitan areas based on need, he added. “The money goes where the epidemic is.”
The largest part of the Ryan White Program is Part B that supports states and territories to provide HIV care, mainly for the AIDS Drug Assistance program. The Part C program supplements funding to metropolitan areas and states and territories to ensure that clinical capacity exists to serve people with HIV in all parts of the country. One issue that worries HIV professionals involved in the program is the executive order that prohibits transgender care because many are at increased risk for or have HIV, Mr. Crowley noted. “We cannot end the epidemic if we ignore a part of the population of people with HIV,” he said.
Part F is proposed for elimination. This includes the AIDS Education and Training Center Program, which trains doctors, nurses and other medical professionals to provide high-quality HIV care. “Where do you think all these primary care providers are learning about HIV care? It’s these AIDS education centers,” he said. This is a part of the program that Mr. Kennedy intends to close, according to his budget brief.
“These are really challenging, but hopeful times,” Mr. Crowley said. “This is not the time to gut the things that we’ve spent decades working on.”
Most of the sources have received funding for HIV research.
Update on this issue:
Federal District Judge William G. Young ruled that hundreds of grants terminated by the National Institutes of Health were "void and illegal," and he ordered that some of them be reinstated. Calling the reasons for grant termination were "arbitrary and capricious," he ordered that grants related to two lawsuits that challenged their cancellation be reinstated. There has been no word on whether the NIH will appeal.
This article is from the June 2025 print issue.