

Over the past 2 decades, the strides made in HIV public health programs, antiretroviral therapy, and care delivery have been nothing short of miraculous—progress once deemed unimaginable. However, the distribution of this progress in the United States has been far from equitable. The HIV epidemic endures, is particularly entrenched in the southern United States, and disproportionately affects marginalized groups, including Black/African American and Hispanic/Latino individuals, men who have sex with men (MSM), other gender and sexual minorities, and people who inject drugs.1 These key populations suffer deep-seated disparities within the HIV care continuum, highlighting significant areas for targeted action.
One major driver of these inequities is the detrimental impact of racism in healthcare, recognized by the CDC as a public health threat.2 In addition to racism, homophobia, transphobia, and stigma exacerbate both physical and mental health problems and impede access to high-quality, culturally competent health services spanning prevention, diagnosis, and treatment. Addressing disparities requires acknowledging these factors and confronting the critical role played by social determinants of health and syndemics that continue to shape the HIV epidemic. These include income, education, housing, immigration status, insurance coverage, drug use, mental health, and geographic region. Simply possessing effective tools is insufficient; they must reach vulnerable populations equitably through a systems-based, multipronged approach.
The Ending the HIV Epidemic in the US (EHE) initiative, launched by the federal government in 2019, aims to end the HIV epidemic in the country by 2030, with targets of achieving a 75% reduction in new infections by 2025 and 90% by 2030.3 As infectious disease clinicians, it is crucial that we educate ourselves about HIV disparities. Equipping ourselves with a foundational understanding of the state of HIV care inequities empowers us to advocate for change, better support our patients, and collectively achieve the ambitious EHE goals. Enhanced knowledge of disparities enables us to more effectively target key populations for HIV prevention access and retention in care initiatives. This article serves not only as a primer on the state of HIV disparities, but also as a rallying cry to take action and drive advocacy efforts forward.
Disparities in HIV Prevalence and Incidence
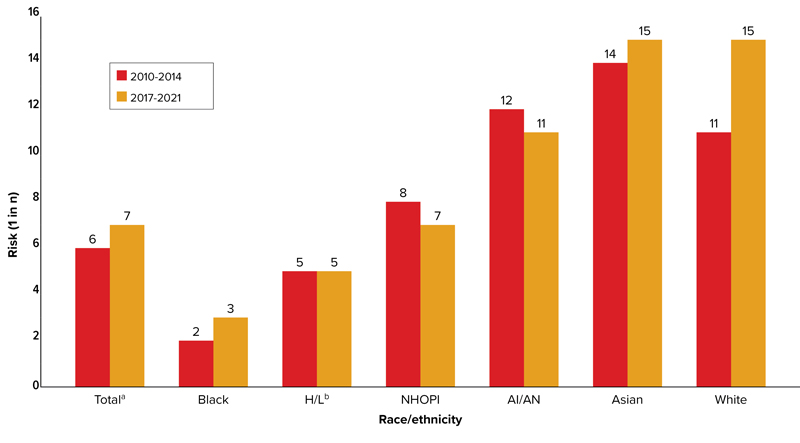
In 2021, the CDC estimated that 32,100 new HIV infections occurred in the United States, bringing the total number of individuals ages 13 years and older living with HIV to 1.2 million.4 Of these, approximately 13% were unaware of their diagnosis. Although gay, bisexual, and other MSM are estimated to constitute approximately 3% to 6% of the adult male population in the United States, they accounted for approximately 70% of these new infections, representing the most affected demographic group and comprising 64% of all people living with HIV in the United States.5 Notably, Black/African American MSM accounted for 25% of all new diagnoses and 36% of diagnoses among MSM. An updated calculation of lifetime risk estimates for receiving an HIV diagnosis, presented by the CDC at CROI 2024, underscored the intersection of race/ethnicity and sexual orientation/behavior in compounding these disparities. The analysis revealed a lifetime risk for HIV acquisition of 1 in 7 among MSM overall, with higher risks of 1 in 3 for Black MSM, 1 in 5 for Hispanic/Latino MSM, 1 in 7 for Native Hawaiian/other Pacific Islander individuals, 1 in 11 for American Indian/Alaska Natives, and 1 in 15 for Asian individuals and White individuals (Figure 1).6 Transgender individuals, particularly transgender women, are also significantly affected by HIV, experiencing high levels of HIV stigma and barriers to care, which highlights the necessity for targeted interventions and culturally competent care for this community.3
The most significant disparities in HIV diagnoses in the United States are observed between Black and White individuals.7 While Black/African Americans account for approximately 12% of the US population, they represent 40% of the new infections, whereas Whites, constituting 61% of the population, account for 26% of new infections (Figure 2). Disparities also exist among women, with the rate of new HIV infections in Black women being approximately 10 times that in White women.
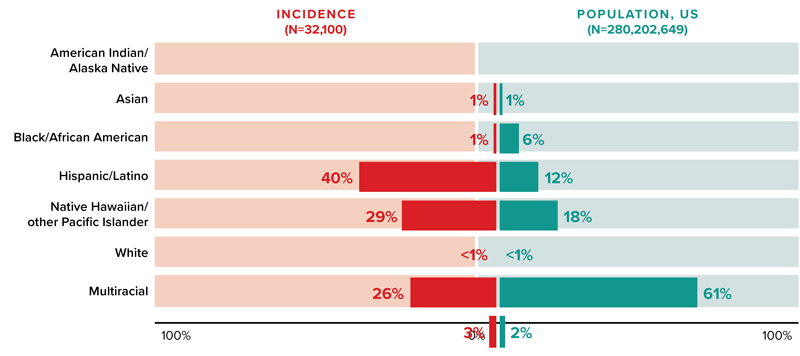
Another noteworthy disparity pertains to Hispanic/Latino individuals, who comprise 18% of the population but represent 29% of new infections. Many Hispanic/Latino people face barriers to accessing quality, culturally competent, and language-concordant prevention, testing, and treatment services. One other significant trend in HIV incidence is the rising contribution of injection drug use to the statistics of new infections, accounting for approximately 8% of new infections in 2021, according to the CDC.
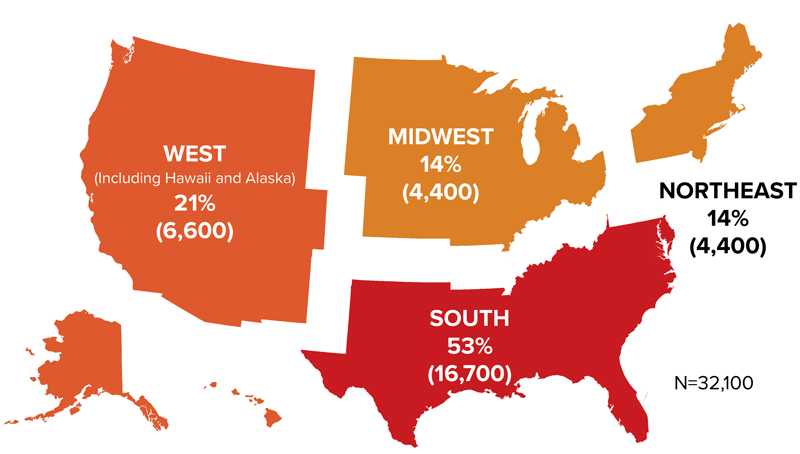
The southern United States persists as the focal point of the epidemic, accounting for 52% of new infections—more than all other regions combined—despite being home to just 38% of the population (Figure 3).1 This disparity underscores the multifaceted challenges fueling the southern epidemic. Socioeconomic factors, including lower household income, increased rates of poverty, more limited insurance coverage, extended travel distances to access care, reduced availability of services, and stigma collectively contribute to the region’s increased vulnerability. Yet it is alarming to note that 7 of the 10 states that have not expanded Medicaid—a vital lifeline and the largest source of health coverage for people with HIV across the nation—are in the South.8
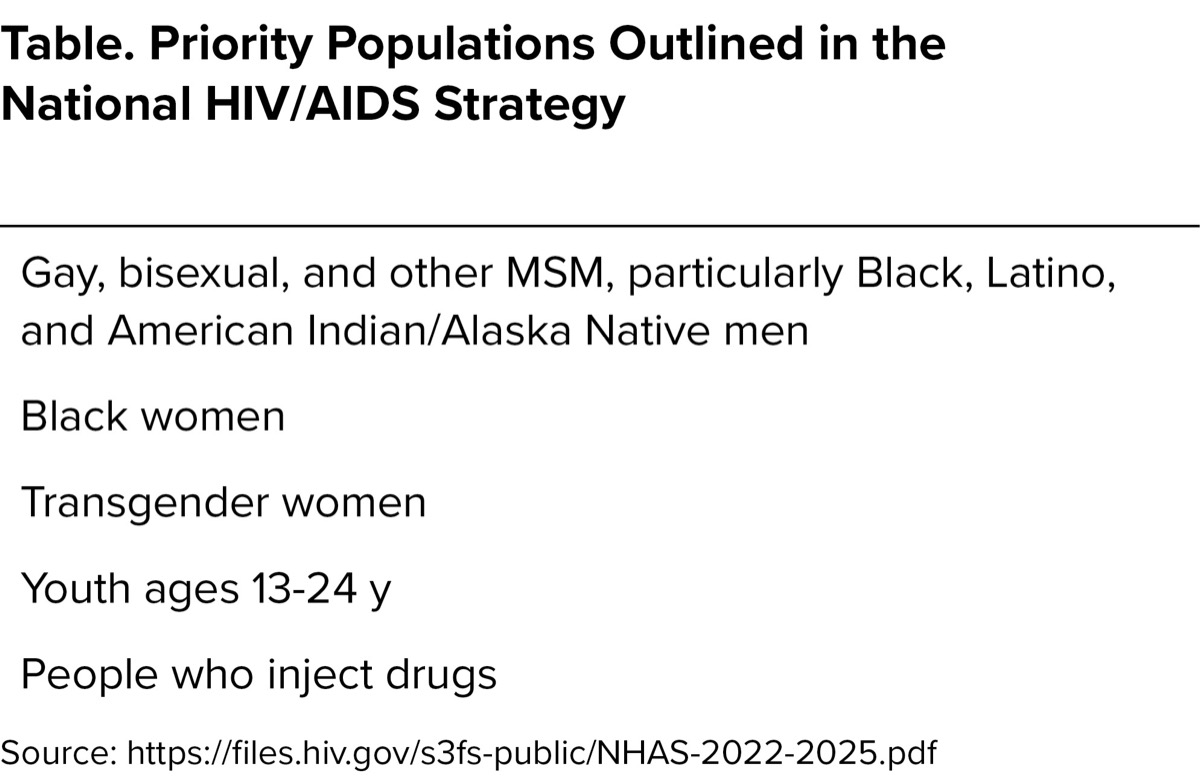
Recognizing how HIV disproportionally affects certain populations, the National HIV/AIDS Strategy designated 5 priority populations: gay, bisexual, and other MSM, particularly, Black, Latino, and American Indian/Alaska Native men; Black women; transgender women; youth ages 13 to 24 years; and people who inject drugs (Table).9
| Table. Priority Populations Outlined in the National HIV/AIDS Strategy |
| Gay, bisexual, and other MSM, particularly Black, Latino, and American Indian/Alaska Native men |
| Black women |
| Transgender women |
| Youth ages 13-24 y |
| People who inject drugs |
| Source: https://files.hiv.gov/s3fs-public/NHAS-2022-2025.pdf |
The Role of the Clinician
How can we help? What is the role of the clinician at the point of care? In considering our individual roles as infectious disease clinicians, it is natural to feel overwhelmed by the magnitude of HIV disparities. However, it is crucial to understand that meaningful change stems from collective action. Even the smallest initiatives within our local clinics and hospitals can yield significant results in reducing disparities within our communities.
To this end, there are several actionable steps we can take.9
Clinicians should prioritize prevention by developing culturally sensitive messaging with local communities most affected by HIV. Engaging in outreach initiatives with community organizations allows us to tailor our messages effectively, ensuring they resonate with diverse populations. This may include delivering messages in multiple languages and meeting people where they are.
Enhancing access to HIV pre-exposure prophylaxis (PrEP) within our settings and addressing PrEP prescription disparities is another vital step, acknowledging that Black MSM are the least likely group of MSM to have been offered HIV PrEP.11 Collaborating with non–infectious disease clinicians, such as primary care physicians and obstetrics/gynecology specialists, empowers them to prescribe PrEP,10 thereby increasing uptake and augmenting HIV prevention efforts.
Furthermore, increasing HIV testing and closing testing gaps within our institutions through quality improvement projects can drive progress. Leveraging partnerships with departments such as the emergency department and obstetrics/gynecology may enable streamlined testing processes and improve diagnosis rates by capitalizing on contact with the healthcare system as a testing opportunity for a wider group of patients.
Recognizing the effects of social determinants of health on patient engagement and retention in care, we must do better to address the needs of people with HIV who use drugs. This may involve collaborating in a multidisciplinary team or advocating for more resources to support substance use treatment, harm reduction strategies, and other services within our practice.
Diversifying the HIV health workforce also is crucial. By recruiting staff who mirror the diversity of our patient populations, we foster a more inclusive and culturally competent care environment. Providing HIV services in languages spoken by our patients and ensuring that staff is sensitive to the needs of gender and sexual minority patients, from registration to consultation, is essential in supporting patients. A large body of evidence has been published about effective linkage to HIV care strategies.12 Patients who are lost to follow-up may benefit from outreach and focused case management services.
Finally, engaging policymakers at the institutional, local, state, and federal levels is essential for sustaining our efforts to combat the epidemic and to eliminate disparities.
As infectious disease clinicians, we wield influential voices that can shape HIV care and prevention initiatives. Let us stand united in our commitment to equality, justice, and unwavering support of our patients. Together, we possess the power to drive meaningful change, eliminate barriers, and create a future where every person affected by HIV receives the care and respect they deserve.
References
- Centers for Disease Control and Prevention. HIV Surveillance Supplemental Report. 2023;28(3). https://bit.ly/4bIdbyl-idse
- Centers for Disease Control and Prevention. Accessed June 4, 2024. https://bit.ly/3R9IGZT-idse
- Centers for Disease Control and Prevention. Accessed June 4, 2024. https://bit.ly/4bcvWJK-IDSE
- Centers for Disease Control and Prevention. Accessed June 4, 2024. https://bit.ly/4e8TX6p-IDSE
- Lieb S, Fallon SJ, Friedman SR, et al. Public Health Rep. 2011;126(1):60-72.
- Singh S. Presented at CROI 2024; March 3-6, 2024; Denver, CO. Abstract 193.
- Hess KL, Xiaohong H., Lansky A, et al. Ann Epidemial. 2017;27(4):238243.
- Dailey A. Presented at CROI 2024; March 3-6, 2024; Denver, CO. Abstract 192.
- KFF. Status of state Medicaid expansion decisions: interactive map. Accessed June 4, 2024. https://bit.ly/4e8dJiI-IDSE
- Office of National AIDS Policy. Accessed June 4, 2024. https://www.hiv.gov/federal-response/national-hiv-aids-strategy/national-hiv-aids-strategy-2022-2025
- Ezennia O, Geter A, Smith DK. AIDS Behav. 2019;23(10):2654-2673.
- Centers for Disease Control and Prevention. Accessed June 2, 2024. https://www.cdc.gov/hiv/effective-interventions/treat/artas/index.html
About the author:

Copyright © 2024 McMahon Publishing, 545 West 45th Street, New York, NY 10036. Printed in the USA. All rights reserved, including the right of reproduction, in whole or in part, in any form.

Download to read this article in PDF document:![]() Spotlighting Disparities: Ongoing Challenges in US HIV Care
Spotlighting Disparities: Ongoing Challenges in US HIV Care