

Over the past few decades, HIV care has improved substantially. Earlier initiation of antiretroviral therapy (ART) and better medication options have resulted in a narrowing in the mortality gap between people with and without HIV. In fact, people with HIV (PWH) now have a near-normal life expectancy. Nevertheless, important challenges persist, including the fact that a subset of PWH struggle with adherence to oral daily treatment; for these individuals, long-acting injectable ART combined with intensive support may be lifesaving. Moreover, PWH continue to have an elevated risk for non–AIDS-related comorbidities, such as cardiovascular disease (CVD), in part associated with persistent inflammation despite virologic suppression.
Recent advances include the demonstration that statins reduce cardiovascular events in PWH. This review highlights major updates in HIV management, including when to initiate ART, antiretroviral treatment options, cardiometabolic complications, and preventive care, including vaccines.
Closing the Survival Gap
People with HIV now have a mortality rate that is similar to people without HIV. A U.S. cohort study of approximately 82,000 adults entering HIV care between 1999 and 2017 revealed a marked decline in five-year mortality over time. By 2017, the difference in mortality between PWH and the general population narrowed to 2.7 percentage points, largely due to earlier therapy and improved antiretroviral regimens.1 However, when we discuss remaining challenges, we will return to the mortality gap between people with and without HIV.
The Case for Early ART Initiation
The START (Strategic Timing of AntiRetroviral Treatment) trial provided definitive evidence of the benefit of early initiation of ART.2 Among people with CD4+ counts of more than 500 cells/mcL, immediate ART reduced the incidence of AIDS-related and non-AIDS events compared with deferring treatment. Long-term follow-up of participants in the START trial continue to show the benefit of early ART initiation.3 These findings led the International Antiviral Society (IAS)-USA and the Department of Health and Human Services (HHS) HIV Treatment Guidelines to recommend initiation of ART for PWH, regardless of CD4+ cell count.4,5
When to Start ART in People With OIs and Cancers
The IAS-USA guidelines provide updated recommendations for when to initiate ART in people with opportunistic conditions.4 ART timing is listed in Table 1. If a PWH has an opportunistic infection (OI) for which there is no effective antimicrobial therapy, such as John Cunningham virus–associated progressive multifocal leukoencephalopathy, then ART should be started immediately because it is the only treatment for the OI. For other OIs, such as pneumocystis pneumonia, ART should be started as soon as the patient is tolerating the OI treatment and certainly within 2 weeks of initiating OI therapy.
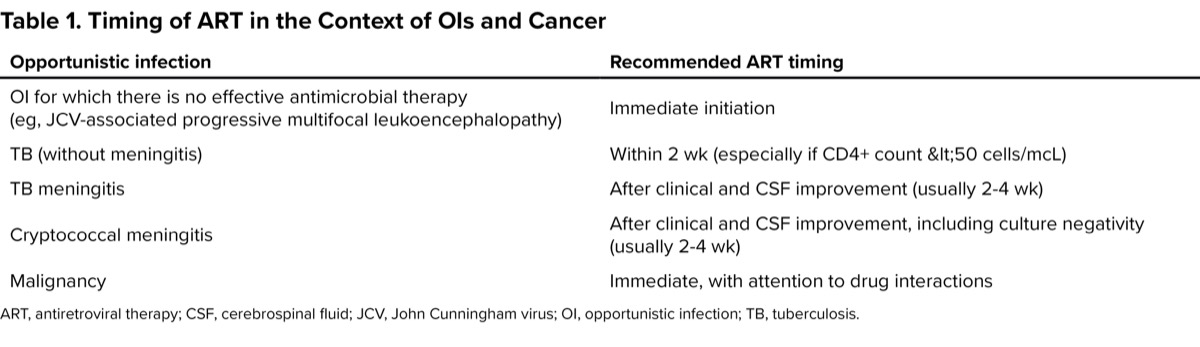
| Table 1. Timing of ART in the Context of OIs and Cancer | |
| Opportunistic infection | Recommended ART timing |
|---|---|
| OI for which there is no effective antimicrobial therapy (eg, JCV-associated progressive multifocal leukoencephalopathy) | Immediate initiation |
| TB (without meningitis) | Within 2 wk (especially if CD4+ count <50 cells/mcL) |
| TB meningitis | After clinical and CSF improvement (usually 2-4 wk) |
| Cryptococcal meningitis | After clinical and CSF improvement, including culture negativity (usually 2-4 wk) |
| Malignancy | Immediate, with attention to drug interactions |
| ART, antiretroviral therapy; CSF, cerebrospinal fluid; JCV, John Cunningham virus; OI, opportunistic infection; TB, tuberculosis. | |
For people with tuberculosis who do not have meningitis, ART should be started within 2 weeks of initiating anti-TB therapy, especially if the CD4+ count is less than 50 cells/mcL. For people with TB or cryptococcal meningitis, ART should be started when the meningitis is improving based on clinical and cerebrospinal fluid (CSF) criteria (including culture conversion in people with cryptococcal meningitis), which is generally 2 to 4 weeks after starting antimicrobial treatment. Finally, patients with malignancies should start ART immediately with careful consideration of drug interactions between ART and the cancer treatment.
Recommended Initial Regimens
The current standard of care is integrase strand transfer inhibitor (INSTI)-based regimens due to their potency, safety, and high barrier to resistance.4,5 These and other regimens are listed in Table 2. Preferred options include bictegravir/emtricitabine/tenofovir alafenamide (BIC/FTC/TAF), and dolutegravir (DTG) combined with either TAF or tenofovir disoproxil fumarate (TDF) and FTC or lamivudine (3TC).
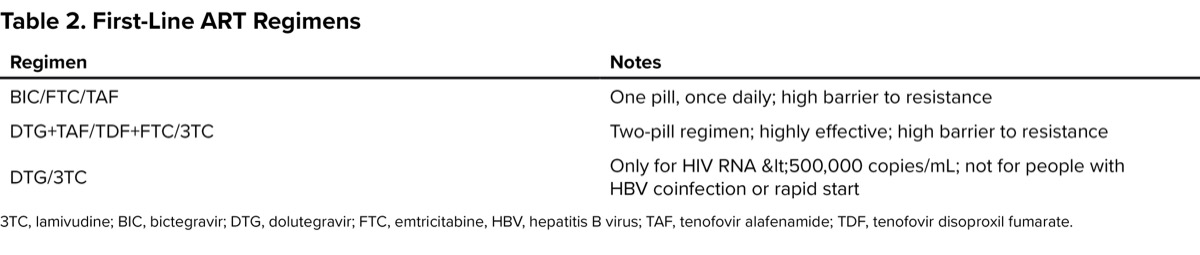
| Table 2. First-Line ART Regimens | |
| Regimen | Notes |
|---|---|
| BIC/FTC/TAF | One pill, once daily; high barrier to resistance |
| DTG+TAF/TDF+FTC/3TC | Two-pill regimen; highly effective; high barrier to resistance |
| DTG/3TC | Only for HIV RNA <500,000 copies/mL; not for people with HBV coinfection or rapid start |
| 3TC, lamivudine; BIC, bictegravir; DTG, dolutegravir; FTC, emtricitabine, HBV, hepatitis B virus; TAF, tenofovir alafenamide; TDF, tenofovir disoproxil fumarate. | |
DTG/3TC is an option for people who do not have hepatitis B virus (HBV) coinfection, do not have baseline resistance to 3TC, and whose HIV RNA is less than 500,000 copies/mL. Because HIV genotyping and HBV testing results usually are not available at the time ART is initiated, many experts start 3-drug therapy and then consider stepping down to DTG/3TC when the HIV RNA is suppressed (unless someone has HBV coinfection or 3TC resistance).
ART in Pregnancy
Treatment guidelines recommend the use of DTG+FTC/TAF (or FTC/TDF if FTC/TAF is not available) during pregnancy. If a person previously received cabotegravir for preexposure prophylaxis, then darunavir/ritonavir plus FTC/TAF or FTC/TDF should be used instead because of concern for integrase inhibitor resistance.
Related Content



There are accumulating data in support of the safety and efficacy of BIC/FTC/TAF during pregnancy. Even though bictegravir levels are lower during pregnancy, they remain high enough to suppress HIV replication. For this reason, if a person is found to be pregnant while taking suppressive BIC/FTC/TAF, guidelines recommend continuing that regimen.
By contrast, long-acting injectable cabotegravir/rilpivirine (CAB+RPV) currently is not recommended during pregnancy due to concerns about drug levels and limited safety and efficacy data. In addition, other 2-drug regimens are not recommended during pregnancy.
Long-Acting Injectable ART: CAB+RPV
Injectable CAB+RPV is an option for patients who are virologically suppressed, do not have resistance to either drug, and who do not want to take a daily oral pill.4,5 Long-acting CAB+RPV administered every 2 months was found to be noninferior to standard oral ART in the ATLAS, FLAIR, and ATLAS-2M trials. Patient satisfaction with injectable regimens was high, although virologic failure occurred in approximately 1.4% of participants.
Risk factors for virologic failure while taking CAB+RPV include obesity; certain HIV subtypes (A6), which are more common in Eastern Europe; and RPV resistance mutations detected on proviral genotyping.6
Long-acting ART has been a game changer for people who struggle to take daily oral ART. In the LATITUDE study,7 participants with adherence difficulties received conditional economic incentives to achieve viral suppression with oral therapy before being randomized to monthly injectable CAB+RPV or continued daily oral ART. Those who were switched to injectable ART had higher viral suppression rates than those who remained on oral regimens. This finding highlights that long-acting formulations, when combined with intensive support, may be a transformative strategy for treating people who have difficulty taking daily oral treatment.
Keeping People With HIV Healthy: CV Risk and Statins
Although the mortality difference between PWH and those without HIV has narrowed, there continues to be a gap.8 This gap is related to social determinants of health and other risk factors: PWH are more likely to be poor, have a substance use disorder, and smoke than people without HIV. In addition, PWH have persistent inflammation despite virologic suppression on ART. In fact, high levels of inflammation before ART are correlated with high levels while on ART9—an “immune dysregulation legacy effect.” Persistent inflammation has been linked to CVD and other comorbidities.
Based on the recognition that CVD is prevalent in PWH, the REPRIEVE trial randomized more than 7,700 PWH who were 40 to 75 years of age and who had a low to moderate CV risk (median atherosclerotic CVD [ASCVD], about 5%) to receive pitavastatin or placebo.10 The group that received pitavastatin had a 35% lower incidence of major adverse CV events (such as myocardial infarction) than the group that received placebo. Based on these results, guidelines recommend the use of statins in PWH who are 40 years of age or older and who have an ASCVD risk of 5% or greater. Statins should be considered for PWH who are 40 years of age or older and who have a lower ASCVD risk, particularly if they have HIV-related risk factors for CVD, such as low CD4+ cell count nadir, long duration of uncontrolled viremia, prior use of ART with cardiometabolic side effects, or hepatitis C virus coinfection (Table 3).

| Table 3. Recommendations for Statin Use in People With HIV | |
| Patient group | Statin recommendation |
|---|---|
| Age >40 y, ASCVD risk =5% | Strongly recommended (pitavastatin, atorvastatin, or rosuvastatin) |
| Age >40 y, ASCVD risk <5% with HIV-related risk factors (see page 40) | Consider statin, discuss potential benefit |
| Age 40-75 y with diabetes | Statin indicated |
Weight Gain and GLP-1 Receptor Agonists
Excessive weight gain following ART initiation may occur in PWH, and is more common in female and Black patients, often manifesting within the first year of treatment. Studies have linked weight gain to use of integrase inhibitors and TAF. However, studies of changing ART regimens have not shown an ameliorating effect on weight gain. As a result, ART regimen changes are not recommended in people with excessive weight gain.4 Instead, lifestyle changes and use of drugs such as glucagon-like peptide-1 (GLP-1) receptor agonists are the mainstay of managing excessive weight gain in PWH. Drugs such as semaglutide (Ozempic and Wegovy, Novo Nordisk) have shown promise in reducing hepatic steatosis, visceral adiposity, and total fat in PWH.11,12 However, they also reduce lean body mass, raising concerns for individuals with sarcopenia or lipoatrophy. Weight regain after stopping semaglutide is common, highlighting the need for long-term strategies.
Vaccination in HIV
People with HIV should receive routine vaccinations.13 If the CD4+ count is less than 200 cells/mcL, live-attenuated vaccines should be avoided. In people who are newly diagnosed with HIV, vaccines usually should be administered once the HIV RNA is suppressed on ART. Influenza vaccine should be administered even while starting ART during influenza season. COVID-19 vaccines should also be administered even as ART is started if a person is not up-to-date.
Hepatitis B vaccination guidelines have recently changed to recommend the CpG-adjuvanted HepB vaccine (Heplisav-B, Dynavax), which results in higher rates of seroprotective antibody responses than the older alum-adjuvanted HepB vaccine. Before a person with HIV is switched to a tenofovir-sparing regimen, such as CAB/RPV, it is important to confirm that they are immune to HBV, and if not, administer the HepB vaccine.
Looking Forward
While HIV therapy has achieved remarkable success, ongoing efforts must focus on earlier diagnosis, improved access to care, and addressing social determinants of health. National and global disparities in HIV prevalence persist and must be addressed. Continued research into long-acting antiretroviral agents, viral hepatitis, comorbidities, and curative strategies are critical to improving the care of people living with HIV.
References
- Edwards JK, Cole SR, Breger TL, et al. Mortality among persons entering HIV care compared with the general U.S. population: an observational study. Ann Intern Med. 2021;174(9):1197-1206.
- INSIGHT START Study Group; Lundgren JD, Babiker AG, Gordin F. The initiation of antiretroviral therapy in early asymptomatic HIV infection. N Engl J Med. 2015;373(9):795-807.
- INSIGHT START Study Group; Lundgren JD, Babiker AG, Sharma S. Long-term benefits from early antiretroviral therapy in HIV infection. NEJM Evid. 2023;2(3):10.1056/evidoa2200302.
- Gandhi RT, Landovitz RJ, Sax PE, et al. Antiretroviral drugs for treatment and prevention of HIV in adults: 2024 recommendations of the International Antiviral Society–USA panel.JAMA. 2024;333(7):609-628.
- US Department of Health and Human Services Guidelines. 2024. clinicalinfo.hiv.gov
- Orkin C, Shapiro JM, Perno CF, et al. Expanded multivariable models to assist patient selection for long-acting cabotegravir + rilpivirine treatment: clinical utility of a combination of patient, drug concentration, and viral factors associated with virological failure. Clin Infect Dis. 2023;77(10):1423-1431.
- Rana A, et al. Long-acting injectable CAB/RPV is superior to oral ART in PWH with adherence challenges: ACTG A5359. Abstract 212. Presented at: CROI 2024; March 3-6, 2024; Denver, CO.
- Edwards JK, Cole SR, Breger TL, et al. Five-year mortality for adults entering human immunodeficiency virus care under universal early treatment compared with the general US population. Clin Infect Dis. 2022;75(5):867-874.
- Gandhi RT, McMahon DK, Bosch RJ, et al. Levels of HIV-1 persistence on antiretroviral therapy are not associated with markers of inflammation or activation. PLoS Pathog. 2017 Apr 20. doi.org/10.1371/journal.ppat.1006285
- Grinspoon SK, Fitch KV, Zanni MV, et al. Pitavastatin to prevent cardiovascular disease in HIV infection. N Engl J Med. 2023;389(8):687-699.
- Lake JE, Kitch DW, Kantor A, et al. The effect of open-label semaglutide on metabolic dysfunction–associated steatotic liver disease in people with HIV. Ann Intern Med. 2024;177(6):835-838.
- Eckard AR, Wu Q, Sattar A, et al. Once-weekly semaglutide in people with HIV-associated lipohypertrophy: a randomised, double-blind, placebo-controlled, phase 2b single-centre clinical trial. Lancet Diabetes Endocrinol. 2024;12(8):523-534.
- US Department of Health and Human Services. HIV Clinical Guidelines: Adult and Adolescent Opportunistic Infections. Immunizations for Preventable Diseases in Adults and Adolescents with HIV. Accessed June 2, 2024. clinicalinfo.hiv.gov/en/guidelines/hiv-clinical-guidelines-adult-and-adolescent-opportunistic-infections/
About the author:

Copyright © 2025 McMahon Publishing, 545 West 45th Street, New York, NY 10036. Printed in the USA. All rights reserved, including the right of reproduction, in whole or in part, in any form.

Download to read this article in PDF document:![]() State of the ART: HIV Management in 2025
State of the ART: HIV Management in 2025