

Multidrug-resistant (MDR) and extensively drug-resistant (XDR) Pseudomonas aeruginosa is a prevalent and challenging nosocomial pathogen. According to the International Network for Optimal Resistance (INFORM) monitoring database, their prevalence is high at 11.5% to 24.7% and 9.0% to 11.2%, respectively (Diagn Microbiol Infect Dis 2018;92[1]:69-74).
The World Health Organization designated carbapenem-resistant P. aeruginosa a critical pathogen in substantial need of new therapies to counteract this imminent public health crisis of resistance (Lancet Infect Dis 2018;18[3]:318-327).
Implications of MDR P. aeruginosa
The CDC classified MDR Pseudomonas a serious health threat. Annually in this country, the pathogen accounts for 32,600 cases and 2,700 deaths, plus $767 million in attributable healthcare costs, according to the agency. A U.S. national database study found that patients with MDR P. aeruginosa respiratory infections had higher mortality, approximately seven days longer hospital length of stay (LOS), higher readmission rates and $20,000 excess cost per infection compared with those without an MDR Pseudomonas infection (J Hosp Infect 2019;103[2]:134-141).
“In patients with MDR Pseudomonas, ceftazidime-avibactam [CZA; Avycaz, AbbVie] treatment has been associated with favorable health outcomes versus historical best available therapy,” said Ashlan J. Kunz Coyne, PharmD, MPH, a pharmacokinetics/pharmacodynamics (PK/PD) and health outcomes postdoctoral research fellow in the Anti-Infective Research Laboratory of the Department of Pharmacy Practice, Eugene Applebaum College of Pharmacy and Health Sciences, Wayne State University, in Detroit.

“When it comes to serious infections, the early initiation of effective therapy is critical; however, the impact of time to ceftazidime-avibactam initiation on outcomes is unknown,” Dr. Kunz Coyne added. She and her colleagues sought to evaluate outcomes of pneumonia patients with MDR Pseudomonas receiving early versus late CZA.
Is Earlier Treatment Better?
A multicenter, retrospective cohort study included hospitalized adult patients from 2019 to 2022, who were symptomatic with culture-positive MDR Pseudomonas pneumonia receiving early versus late CZA as the first beta-lactam with in vitro activity, according to a poster (2270) presented at ECCMID 2023, held in Copenhagen.
“We defined early CZA administration to be within 48 hours of culture collection and late to be after 48 hours. The primary outcome analyzed was a composite of clinical success, defined as the absence of all-cause mortality or microbiological recurrence requiring therapy within 30 days from the end of CZA therapy and continued infectious signs/symptoms during CZA therapy,” Dr. Kunz Coyne said.
For the statistical analyses, the study used descriptive statistics for patient and clinical characteristics, a bivariate analysis to compare outcomes between early and late CZA, and logistic regression to account for confounding variables.
A total of 115 patients were included, with 45 receiving early treatment and 70 receiving late treatment. The median age of the patients was 62 years, more than 60% were men, and approximately 80% were admitted to the ICU within 24 hours of CZA initiation. The proportion of patients who received appropriate CZA was similar in early and late groups (91.1% vs. 88.6%, respectively; P=0.218). Clinical success occurred in 77.8% of early patients (35/45) and 60% of late patients (42/70) (P=0.048). The early CZA group had a shorter hospital and an ICU LOS than the late CZA group (15 and nine vs. 32 and 16 days; P<0.004 and P<0.012, respectively). Early CZA was an independent predictor of clinical success on logistic regression analysis (Table).
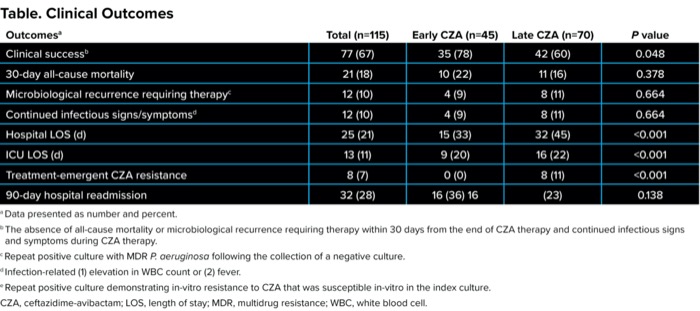
| Table. Clinical Outcomes | ||||
| Outcomesa | Total (n=115) | Early CZA (n=45) | Late CZA (n=70) | P value |
|---|---|---|---|---|
| Clinical successb | 77 (67) | 35 (78) | 42 (60) | 0.048 |
| 30-day all-cause mortality | 21 (18) | 10 (22) | 11 (16) | 0.378 |
| Microbiological recurrence requiring therapyc | 12 (10) | 4 (9) | 8 (11) | 0.664 |
| Continued infectious signs/symptomsd | 12 (10) | 4 (9) | 8 (11) | 0.664 |
| Hospital LOS (d) | 25 (21) | 15 (33) | 32 (45) | <0.001 |
| ICU LOS (d) | 13 (11) | 9 (20) | 16 (22) | <0.001 |
| Treatment-emergent CZA resistance | 8 (7) | 0 (0) | 8 (11) | <0.001 |
| 90-day hospital readmission | 32 (28) | 16 (36) 16 | (23) | 0.138 |
a Data presented as number and percent. b The absence of all-cause mortality or microbiological recurrence requiring therapy within 30 days from the end of CZA therapy and continued infectious signs and symptoms during CZA therapy. c Repeat positive culture with MDR P. aeruginosa following the collection of a negative culture. d Infection-related (1) elevation in WBC count or (2) fever. e Repeat positive culture demonstrating in-vitro resistance to CZA that was susceptible in-vitro in the index culture. CZA, ceftazidime-avibactam; LOS, length of stay; MDR, multidrug resistance; WBC, white blood cell. | ||||
“We found that in hospitalized adult patients with MDR Pseudomonas pneumonia, early CZA was associated with a higher rate of clinical success and shorter hospital and ICU length of stay compared with late CZA,” Dr. Kunz Coyne said. More studies are warranted to assess the effect of antimicrobial stewardship efforts, including the use of rapid diagnostic tests and regimen optimization on clinical outcomes, she added.
The study results reinforce the importance of early effective antimicrobial therapy for improving clinical outcomes, according to Thomas M. File Jr., MD, MSc, MACP, FIDSA, FCCP, who was not part of the study.
“The challenge to us as clinicians is to be able to decide when we should empirically use the newer, more expensive agents to target the more resistant pathogens, such as cefepime versus ceftazidime-avibactam. As the authors indicate in the conclusion, one possible answer is through rapid diagnostic tests that can identify resistant genes via molecular methods before results of standard antimicrobial susceptibility tests are available,” explained Dr. File, the chair of the Infectious Disease Division and co-director of the antimicrobial stewardship program at Summa Health, in Akron, Ohio. He is also a professor of internal medicine, a master teacher and the chair of the Infectious Disease Section at Northeast Ohio Medical University, in Rootstown, as well as an editorial advisory board member of Infectious Disease Special Edition.
More Data to Come at IDWeek
Dr. Kunz Coyne will be presenting data about early versus late CZA for carbapenem-resistant Enterobacterales (CRE) infections at IDWeek in mid-October, in Boston. In that study, early and late CZA were again defined as drug administration within 48 hours of culture collection and after 48 hours, respectively. Currently, there are 23 medical centers across the five U.S. regions participating in the study.
This study was funded through a collaborative study grant from AbbVie. Dr. Kunz Coyne wanted to acknowledge her co-authors: Kristen Lucas, Paige Witucki, Carolina Orzol, Callan Bleick, Michael J. Rybak, James Truong, Justin Andrade, John Cerenzio, Mark Biagi, Michaela Todd and Michael Veve.


This article is from the August 2023 print issue.