


By David Wild
Expanding inpatient medication stewardship efforts to encompass antiretroviral therapy (ART) can slash medication errors and 30-day hospital readmission rates by more than 50% in people living with HIV, recent studies suggest.
“ARVSPs [antiretroviral stewardship programs] improve outcomes for patients because they ensure patients get the right medications, at the right time, in the right doses,” said Elizabeth Sherman, PharmD, an associate professor of pharmacy practice at Nova Southeastern University, in Fort Lauderdale, Fla., who helped launch her own institution’s program.
Inpatient medication errors related to ART or opportunistic infection (OI) treatments occur in up to 72% of hospitalized patients with HIV (Open Forum Infect Dis 2020;7[8]:ofaa073), making medication monitoring imperative in this population, Amber Ladak, PharmD, an HIV pharmacist in the Division of Infectious Disease at the Medical College of Georgia at Augusta University, said during a session on ARVSPs at the 2021 annual meeting of the American College of Clinical Pharmacy (ACCP).
“Hospitalized patients with HIV require careful medication review and management, both because of their complex antiretroviral regimens and because they are receiving increasingly more medications for non-HIV comorbidities,” Dr. Ladak said.
Part of the reason the error rate is so high is that many hospitalists do not have expertise in HIV treatment and can make mistakes when initiating or modifying complex HIV regimens, Dr. Ladak said. “There are just so many different combinations of antiretrovirals that it’s quite easy for physicians to start a regimen without a booster, for example, or to prescribe a regimen that doesn’t match the patient’s outpatient treatment,” she explained.
The good news is that pharmacists can help reduce these errors by implementing simple ARVSP interventions. For example, adding clear instructions in computerized physician order entry (CPOE) systems can guide accurate dosing and prompt physicians to double-check the regimen they are prescribing, Dr. Ladak said.
Another low-cost measure that Dr. Ladak and her colleagues have found helpful in mitigating errors for ART orders has been to add brand names alongside single-tablet multidrug treatments in their CPOE system. “If someone is ordering quickly and looking only at the first couple of drugs of a regimen, they can easily confuse it for another regimen,” she said.
Reducing Mix-Ups
Although Dr. Ladak did not share details on the effectiveness of adding brand names to the CPOE system at her institution, she said it has reduced the number of mix-ups between ART treatments that share some of the same components. She also cited data showing CPOE-based tools such as this have reduced inpatient ART-related errors by more than 40% (Clin Infect Dis 2020;70[11]:2241-2246).
Other stewardship tools pharmacists can use include HIV-specific clinical checklists, Dr. Ladak said. Checklists can augment medication reviews at the time of admission and discharge and can be tailored to the specific institution. Common components in use by Dr. Ladak and her colleagues, and described in a 2020 study she co-authored, include patients’ outpatient and inpatient ART and non-ART medications, drug allergies, interactions with non-ART drugs, OI prophylaxis and a review of their most recent HIV viral loads, to verify treatment efficacy (J Int Assoc Provid AIDS Care 2020;19:2325958219898457).
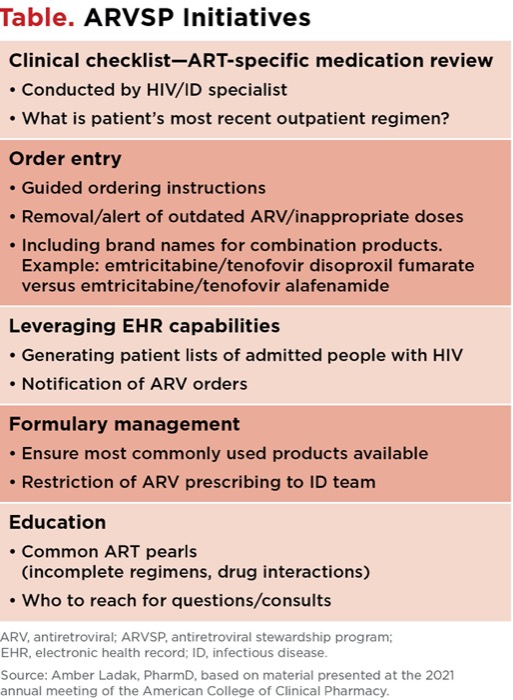
| Table. ARVSP Initiatives |
| Clinical checklist—ART-specific medication review Conducted by HIV/ID specialist What is patient’s most recent outpatient regimen? |
| Order entry Guided ordering instructions Removal/alert of outdated ARV/inappropriate doses Including brand names for combination products. Example: emtricitabine/tenofovir disoproxil fumarate versus emtricitabine/tenofovir alafenamide |
| Leveraging EHR capabilities Generating patient lists of admitted people with HIV Notification of ARV orders |
| Formulary management Ensure most commonly used products available Restriction of ARV prescribing to ID team |
| Education Common ART pearls (incomplete regimens, drug interactions) Who to reach for questions/consults |
| ARV, antiretroviral; ARVSP, antiretroviral stewardship program; EHR, electronic health record; ID, infectious disease. Source: Amber Ladak, PharmD, based on material presented at the 2021 annual meeting of the American College of Clinical Pharmacy. |
In a separate study examining the impact of an ARVSP with a strong emphasis on medication reviews, investigators found that 17% of patients admitted with HIV had medication errors prior to an ARVSP (Open Forum Infect Dis 2020;7[8]:ofaa073). These included omissions of OI treatment or ART, drug–drug interactions and incorrect therapy. After the program’s implementation, the error rate dropped to 6%. All errors were resolved prior to discharge and the 30-day all-cause readmission rate fell from 27% to 12% (P=0.03).
To ensure they don’t miss any opportunity to conduct a thorough medication review and use their checklist, Dr. Ladak said she and her colleagues have set their electronic health record (EHR) to generate a daily list of patients admitted with HIV. They use the checklist at the time of admission and discharge, when they also educate patients on any new medications, document changes to their treatment regimens and contact patients’ outpatient providers to notify them of these changes.
Errors Slashed at Nova Southeastern University
Reviewing thrice-weekly EHR-generated reports of inpatients receiving an ARV has had a profound effect on medication error rates at Nova Southeastern University, noted Dr. Sherman, who served as one of four pharmacists in the nation selected to author the ASHP Guidelines on Pharmacist Involvement in HIV Care (bit.ly/3vEb2kR). Her team implemented their ARVSP in January 2020 and found that the program significantly reduced the number of uncorrected ART errors. Six months before rollout, the error rate was 64% versus 31% six months after implementation (P<0.05) (J Am Pharm Assoc 2022;62[1]:264-269). Moreover, the proportion of patients with at least one medication error fell from 55.5% to 32.6%, reported Dr. Sherman, who was not part of the ACCP session.
Taking It Slow
Institutions interested in launching their own ARVSP can set themselves up for success by implementing the program gradually, Dr. Ladak advised. “Perform a baseline evaluation and identify areas with the greatest need, whether that’s improving medication reviews at the time of admission or educating physicians,” she said. “Focus on one or two stewardship activities first, do them well and then add more activities as needed.”

It is also important to designate a program lead with expertise in HIV or other infectious diseases who can provide oversight, assume responsibility for the ARVSP, spearhead the development of policies and review the program’s results after implementation, Dr. Ladak said. In addition, one of the most important steps the ARVSP program lead can take is to provide prescriber education, she said.
“Sharing ART pearls, educating prescribers about the most common prescribing errors and drug interactions, and providing regular updates on available treatments can go a long way,” Dr. Ladak said.
Dr. Sherman echoed this sentiment, urging institutions that may not have the resources to implement a full ARVSP to focus on education as one way of improving ART use in hospitals. “Educating healthcare staff about clinical pearls and using medication errors as learning lessons, or even just having a dedicated person the staff can call with questions about ARV regimens, can be very helpful in preventing ARV medication errors.”
Dr. Ladak reported serving on an advisory board for Theratechnologies. Dr. Sherman reported no relevant financial disclosures.



This article is from the June 2022 print issue.