

Although rare, mpox breakthrough infection or reinfection can occur whether the person was vaccinated or had the infection, according to two studies presented at CROI 2025, in San Francisco.
However, experts noted that at this time, people with previous infection do not need vaccination.
Waning Immunity
As breakthrough infections in vaccinated people and reports of reinfections have raised questions about immune durability and the need for vaccine boosters, investigators at University College Dublin conducted a prospective cohort study comparing participants with prior mpox infection, vaccination with modified vaccinia virus Ankara (MVA-BN; Jynneos, Bavarian Nordic) and historical controls (abstract 439). The vaccine cohort involved 122 participants, who all identified as male, ranging in age from 33 to 44 years; 25% were people with HIV (PWH) and 11% had prior smallpox vaccination. The mpox cohort included 13 participants, also 100% male, ranging in age from 31 to 40, 23% PWH and 0% with prior smallpox vaccination.
Of those with prior mpox, 85% (11/13) remained seropositive at 747 (677-865) days, reported the researchers, led by Joanne Byrne, a PhD candidate at the university. “In contrast, the mean predicted VACVB5 titers following MVA vaccination fell below the seropositive threshold at 472 (95% CI, 389-587) days, with only 32% (39/122) remaining seropositive at 652 (607-700) days,” they noted. They also found that PWH had significantly lower odds of retaining seropositivity post-vaccination (odds ratio [OR], 0.17; P=0.01), an association that persisted when adjusted for time since vaccination, age and prior smallpox vaccination (adjusted OR, 0.19; P=0.01).
“How these data relate to risk for reinfection or need for booster vaccination remains to be determined,” they said.
Rare Reinfections
In another study, a group of investigators from the California Department of Public Health found that previous mpox infection does not confer long-term immunity in all people (abstract 1092).
The investigators conducted a retrospective descriptive analysis of people who met the definition for mpox reinfection in California as reported by public health surveillance from May 2022 to August 2024. They identified possible mpox reinfection among those with two positive results from polymerase chain reaction (PCR) tests separated by more than 60 days, with medical chart review of all possible reinfections to verify symptom resolution between test results, and classifying cases as suspect, probable or confirmed according to case definition from the CDC.
Out of 6,476 reported mpox cases, nine confirmed/probable mpox reinfections were identified (0.14%). All nine probable/confirmed reinfection cases were cisgender male and gay, bisexual or other men who have sex with men, ranging in age from 26 to 59 years, with five (56%) identifying as Hispanic/Latinx and four (44%) PWH. The time interval from first to second infection ranged from 266 to 778 days (median, 448 days). Three cases had samples available from both infections. In these cases, whole-genome sequencing identified distinct clade IIb mpox virus lineages over time, thereby confirming reinfection (as opposed to persistent infections) per the CDC case definition.
Prior to their first infection, one person had received a single dose of the MVA-BN vaccine; prior to the second infection, two had received a single dose and two had received two doses of the vaccine. The number of sexual partners 21 days before infection ranged from one to 10 for the first infection and one to 15 for the second infection. The study did not include seropositivity (or any analysis of immunity) over time, nor did it analyze time to reinfection.
“Clinicians should consider mpox in all patients with compatible symptoms of mpox, even if the patient has a history of previous mpox infection,” said presenting author Jessica Watson, MD, MPH, a public health medical officer at the California Department of Public Health. She noted that the study’s reinfection rates are likely an underestimate due to undertesting and lack of disease recognition. “More research is needed to understand the risk factors, need for vaccination post-infection and clinical outcomes among people who are infected with mpox multiple times.”
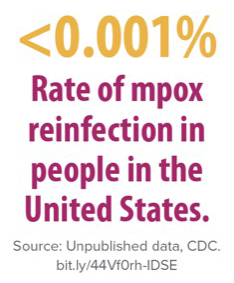
The findings do not, however, suggest that vaccinations are necessary in people who had prior mpox infection, Dr. Watson noted. “Our findings confirm that mpox reinfection is very rare. Existing CDC data show that in instances where an individual did get reinfected, the second illness was generally milder than the first infection. Our study supports current CDC recommendations that people with previous mpox infection are not recommended to receive Jynneos vaccine at this time.”
Drs. Byrne and Watson reported no relevant financial disclosures.

This article is from the June 2025 print issue.